Gastroenterology, Rambam Health Care Campus, Haifa, Israel.
Faculty of Biotechnology and Food Engineering, Technion Israel Institute of Technology, Haifa, Israel.
Gut. 2022 Feb;71(2):287-295. doi: 10.1136/gutjnl-2021-325185. Epub 2021 Aug 3.
Anti-drug antibodies (ADA) to anti-tumour necrosis factor (anti-TNF) therapy drive treatment loss of response. An association between intestinal microbial composition and response to anti-TNF therapy was noted. We therefore aimed to assess the implications of antibiotic treatments on ADA formation in patients with inflammatory bowel disease (IBD).
We analysed data from the epi-IIRN (epidemiology group of the Israeli IBD research nucleus), a nationwide registry of all patients with IBD in Israel. We included all patients treated with anti-TNF who had available ADA levels. Survival analysis with drug use as time varying covariates were used to assess the association between antibiotic use and ADA development. Next, specific pathogen and germ-free C57BL mice were treated with respective antibiotics and challenged with infliximab. ADA were assessed after 14 days.
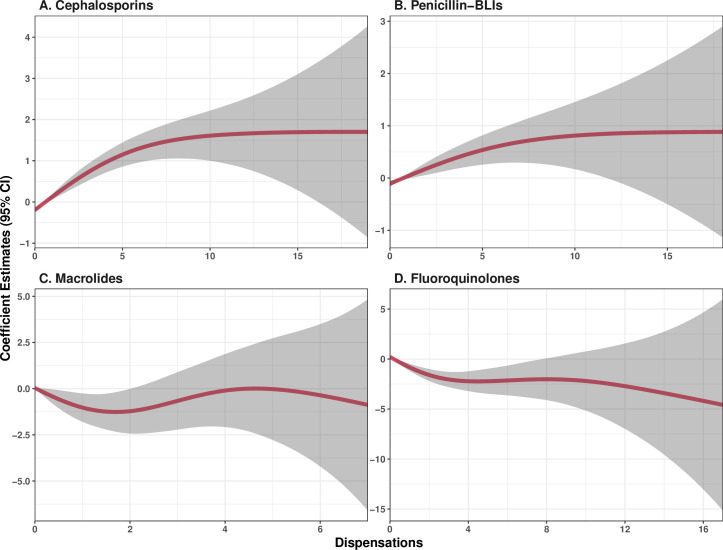
Among 1946 eligible patients, with a median follow-up of 651 days from initiation of therapy, 363 had positive ADA. Cox proportional hazard model demonstrated an increased risk of ADA development in patients who used cephalosporins (HR=1.97, 95% CI 1.58 to 2.44), or penicillins with β-lactamase inhibitors (penicillin-BLI, HR=1.4, 95% CI 1.13 to 1.74), whereas a reduced risk was noted in patients treated with macrolides (HR=0.38, 95% CI 0.16 to 0.86) or fluoroquinolones (HR=0.20, 95% CI 0.12 to 0.35). In mice exposed to infliximab, significantly increased ADA production was observed in cephalosporin as compared with macrolide pretreated mice. Germ-free mice produced no ADA.
ADA production is associated with the microbial composition. The risk of ADA development during anti-TNF therapy can possibly be reduced by avoidance of cephalosporins and penicillin-BLIs, or by treatment with fluoroquinolones or macrolides.
抗肿瘤坏死因子(anti-TNF)治疗的抗药物抗体(ADA)导致治疗应答丧失。有人注意到肠道微生物组成与抗 TNF 治疗应答之间存在关联。因此,我们旨在评估抗生素治疗对炎症性肠病(IBD)患者 ADA 形成的影响。
我们分析了以色列 IBD 研究核(epi-IIRN)的流行病学组(一个以色列所有 IBD 患者的全国性登记处)的数据。我们纳入了所有接受抗 TNF 治疗且 ADA 水平可获得的患者。使用药物使用作为时间变化协变量的生存分析来评估抗生素使用与 ADA 发展之间的关联。接下来,用相应的抗生素处理特定病原体和无菌 C57BL 小鼠,并用英夫利昔单抗对其进行挑战。14 天后评估 ADA。
在 1946 名符合条件的患者中,从开始治疗到中位随访 651 天,363 例 ADA 阳性。Cox 比例风险模型显示,使用头孢菌素(HR=1.97,95%CI 1.58 至 2.44)或青霉素-β-内酰胺酶抑制剂(青霉素-BLI,HR=1.4,95%CI 1.13 至 1.74)的患者 ADA 发展的风险增加,而使用大环内酯类(HR=0.38,95%CI 0.16 至 0.86)或氟喹诺酮类(HR=0.20,95%CI 0.12 至 0.35)的患者风险降低。与用大环内酯预处理的小鼠相比,用头孢菌素处理的小鼠在暴露于英夫利昔单抗后 ADA 的产生明显增加。无菌小鼠未产生 ADA。
ADA 的产生与微生物组成有关。在抗 TNF 治疗期间,通过避免使用头孢菌素和青霉素-BLI,或使用氟喹诺酮类或大环内酯类药物,ADA 发展的风险可能会降低。