Medical Clinic and Policlinic I, Hematology and Cellular Therapy, University Hospital Leipzig, Leipzig, Germany; NCT Trial Center, National Center of Tumor Diseases, German Cancer Research Center (DKFZ), Heidelberg, Germany; Department of Internal Medicine V, Heidelberg University Hospital, Heidelberg.
Department of Medicine I, University Hospital Carl-Gustav-Carus, Dresden.
Haematologica. 2022 Apr 1;107(4):836-843. doi: 10.3324/haematol.2021.278645.
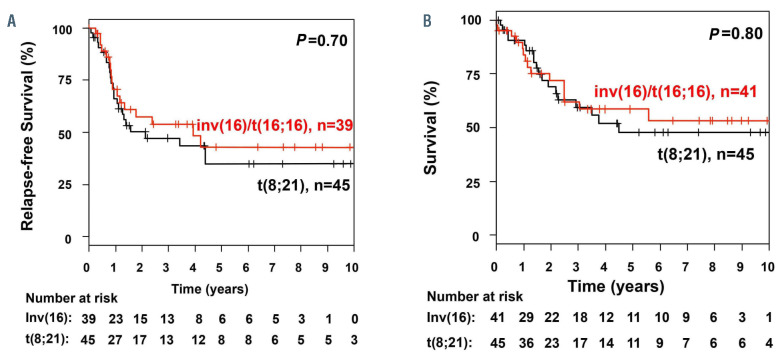
The aim of this study was to evaluate the prognostic impact of FLT3-ITD in core-binding factor acute myeloid leukemia (CBFAML) in an international, multicenter survey of 97 patients of whom 52% had t(8;21)(q22;q22) and 48% had inv(16)(p13q22)/t(16;16)(p13;q22). The median age of the patients was 53 years (range, 19-81). Complete remission after anthracycline-based induction (n=86) and non-intensive therapy (n=11) was achieved in 97% and 36% of the patients, respectively. The median follow-up was 4.43 years (95% confidence interval [95% CI]: 3.35-7.39 years). The median survival after intensive and non-intensive treatment was not reached and 0.96 years, respectively. Among intensively treated patients, inv(16) with trisomy 22 (n=11) was associated with a favorable 4-year relapse-free survival rate of 80% (95% CI: 59-100%) as compared to 38% (95% CI: 27-54%; P=0.02) in all other patients with CBFAML/ FLT3-ITD (n=75). Overall, 24 patients underwent allogeneic hematopoietic cell transplantation (HCT), 12 in first complete remission and 12 after relapse. Allogeneic HCT in first complete remission was not beneficial (P=0.60); however, allogeneic HCT seemed to improve median survival in relapsed patients compared to that of patients treated with chemotherapy (not reached vs. 0.6 years, respectively; P=0.002). Excluding patients with inv(16) with trisomy 22, our data indicate that compathe outcome of CBF-AML patients with FLT3-ITD may be inferior to that of patients without FLT3-ITD (based on previously published data), suggesting that prognostically CBF-AML patients with FLT3-ITD should not be classified as favorable-risk. FLT3-inhibitors may improve the outcome of these patients.
本研究的目的是评估国际多中心 97 例患者中 FLT3-ITD 在伴有核心结合因子(CBF)的急性髓系白血病(CBF-AML)中的预后影响,其中 52%的患者存在 t(8;21)(q22;q22),48%的患者存在 inv(16)(p13q22)/t(16;16)(p13;q22)。患者的中位年龄为 53 岁(范围 19-81 岁)。接受蒽环类药物为基础的诱导(n=86)和非强化治疗(n=11)后,分别有 97%和 36%的患者达到完全缓解。中位随访时间为 4.43 年(95%置信区间[95%CI]:3.35-7.39 年)。强化治疗和非强化治疗后患者的中位生存时间分别为未达到和 0.96 年。在强化治疗的患者中,inv(16)伴三体 22(n=11)的 4 年无复发生存率为 80%(95%CI:59-100%),而所有其他 CBF-AML/FLT3-ITD 患者(n=75)的无复发生存率为 38%(95%CI:27-54%;P=0.02)。总体而言,24 例患者接受了异基因造血细胞移植(HCT),其中 12 例在首次完全缓解时,12 例在复发后。首次完全缓解时接受异基因 HCT 没有益处(P=0.60);然而,与接受化疗的患者相比,异基因 HCT 似乎改善了复发患者的中位生存时间(未达到 vs. 0.6 年,P=0.002)。排除 inv(16)伴三体 22 的患者后,我们的数据表明,FLT3-ITD 伴有 CBF-AML 患者的预后可能不如无 FLT3-ITD 的患者(基于先前发表的数据),提示预后上伴有 FLT3-ITD 的 CBF-AML 患者不应被归类为低危风险。FLT3 抑制剂可能改善这些患者的预后。