Huang Yen-Hsiang, Hsu Kuo-Hsuan, Chin Chun-Shih, Tseng Jeng-Sen, Yang Tsung-Ying, Chen Kun-Chieh, Su Kang-Yi, Yu Sung-Liang, Chen Jeremy J W, Chang Gee-Chen
Division of Chest Medicine, Department of Internal Medicine, Taichung Veterans General Hospital, Taichung, Taiwan.
Institute of Biomedical Sciences, National Chung Hsing University, Taichung, Taiwan.
Cancer Res Treat. 2022 Apr;54(2):434-444. doi: 10.4143/crt.2021.671. Epub 2021 Aug 2.
The aim of this study was to investigate the efficacy of various epidermal growth factor receptor (EGFR)-tyrosine kinase inhibitors (TKIs) plus bevacizumab in advanced EGFR-mutant lung adenocarcinoma patients.
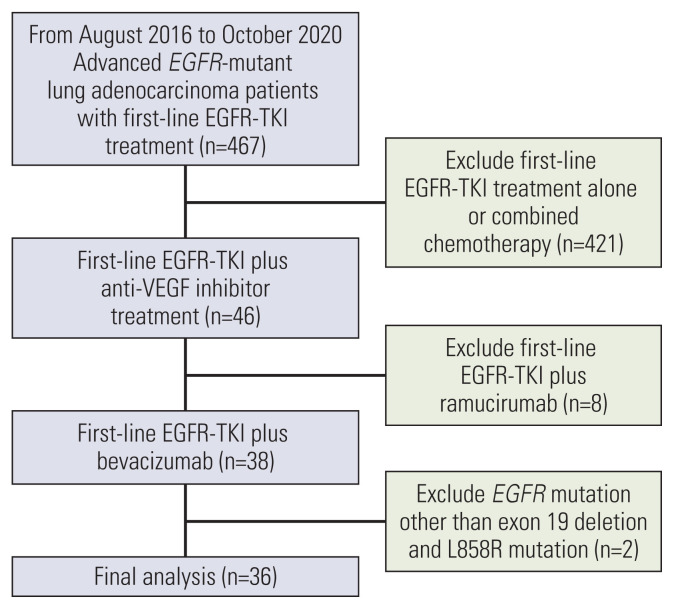
From August 2016 to October 2020, we enrolled advanced lung adenocarcinoma patients harboring exon 19 deletion or L858R receiving gefitinib, erlotinib and afatinib plus bevacizumab as the first-line treatment for the purposes of analysis.
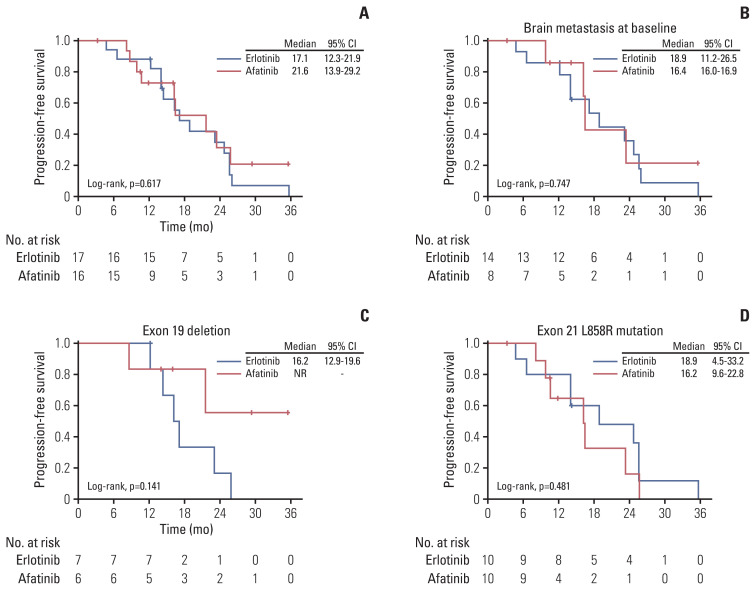
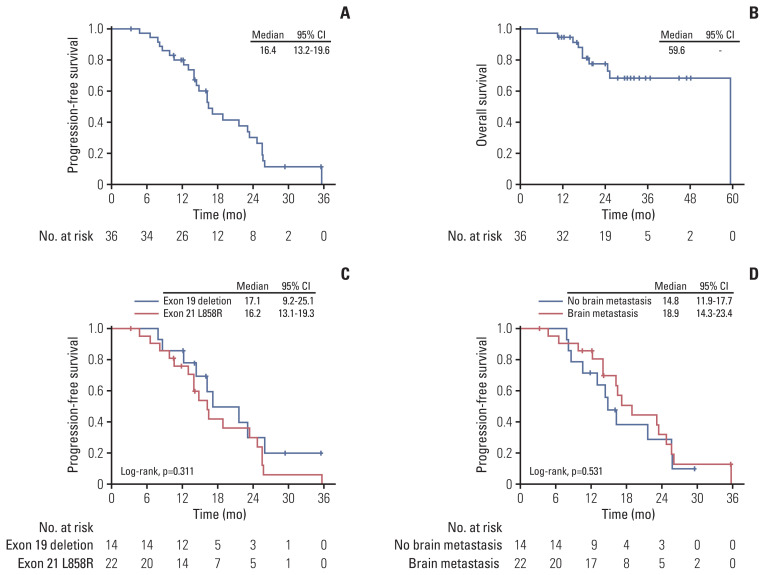
A total of 36 patients were included in the final analysis. Three patients received gefitinib, 17 received erlotinib, and 16 received afatinib combined with bevacizumab as the first-line treatment. The objective response rate was 77.8%, and disease control rate was 94.4%. The overall median progression-free survival (PFS) was 16.4 months, while the median PFS was 17.1 months in patients with exon 19 deletion, and 16.2 months in patients with L858R mutation (p=0.311). Regarding the use of different EGFR-TKIs, the median PFS was 17.1 months in the erlotinib group and 21.6 months in the afatinib group (p=0.617). In patients with brain metastasis at baseline, the median PFS was 18.9 months in the erlotinib group and 16.4 months in the afatinib group (p=0.747). Amongst patients harboring exon 19 deletion, the median PFS was 16.2 months in the erlotinib group and not-reached in the afatinib group (p=0.141). In patients with L858R mutation, the median PFS was 18.9 months in the erlotinib group and 16.2 months in the afatinib group (p=0.481).
Our research demonstrates that not only erlotinib combined with bevacizumab, but also afatinib plus bevacizumab as first-line treatment, provides solid clinical efficacy in advanced EGFR-mutant lung adenocarcinoma patients.
本研究旨在探讨各种表皮生长因子受体(EGFR)-酪氨酸激酶抑制剂(TKIs)联合贝伐单抗治疗晚期EGFR突变型肺腺癌患者的疗效。
2016年8月至2020年10月,我们纳入了携带19外显子缺失或L858R突变的晚期肺腺癌患者,将吉非替尼、厄洛替尼和阿法替尼联合贝伐单抗作为一线治疗方案进行分析。
最终纳入分析的患者共36例。3例患者接受吉非替尼治疗,17例接受厄洛替尼治疗,16例接受阿法替尼联合贝伐单抗作为一线治疗。客观缓解率为77.8%,疾病控制率为94.4%。总体中位无进展生存期(PFS)为16.4个月,其中19外显子缺失患者的中位PFS为17.1个月,L858R突变患者的中位PFS为16.2个月(p=0.311)。就不同EGFR-TKIs的使用情况而言,厄洛替尼组的中位PFS为17.1个月,阿法替尼组为21.6个月(p=0.617)。基线时有脑转移的患者中,厄洛替尼组的中位PFS为18.9个月,阿法替尼组为16.4个月(p=0.747)。在携带19外显子缺失的患者中,厄洛替尼组的中位PFS为16.2个月,阿法替尼组未达到(p=0.141)。在L858R突变患者中,厄洛替尼组的中位PFS为18.9个月,阿法替尼组为16.2个月(p=0.481)。
我们的研究表明,不仅厄洛替尼联合贝伐单抗,而且阿法替尼联合贝伐单抗作为一线治疗,在晚期EGFR突变型肺腺癌患者中均具有可靠的临床疗效。