Department of Intensive Care, Emergency Medicine and Anesthesia, Fondazione Policlinico Universitario A. Gemelli IRCCS, Rome, Italy.
Università Cattolica del Sacro Cuore, Rome, Italy.
Intensive Care Med. 2023 Aug;49(8):934-945. doi: 10.1007/s00134-023-07161-1. Epub 2023 Jul 28.
Although the prevalence of community-acquired respiratory bacterial coinfection upon hospital admission in patients with coronavirus disease 2019 (COVID-19) has been reported to be < 5%, almost three-quarters of patients received antibiotics. We aim to investigate whether procalcitonin (PCT) or C-reactive protein (CRP) upon admission could be helpful biomarkers to identify bacterial coinfection among patients with COVID-19 pneumonia.
We carried out a multicentre, observational cohort study including consecutive COVID-19 patients admitted to 55 Spanish intensive care units (ICUs). The primary outcome was to explore whether PCT or CRP serum levels upon hospital admission could predict bacterial coinfection among patients with COVID-19 pneumonia. The secondary outcome was the evaluation of their association with mortality. We also conducted subgroups analyses in higher risk profile populations.
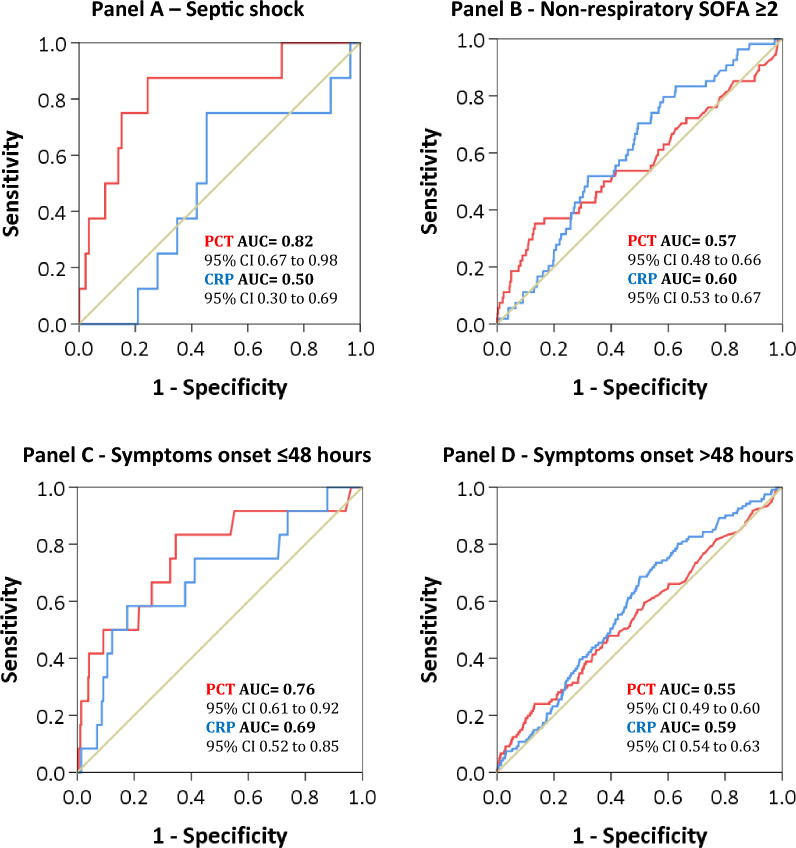
Between 5 February 2020 and 21 December 2021, 4076 patients were included, 133 (3%) of whom presented bacterial coinfection. PCT and CRP had low area under curve (AUC) scores at the receiver operating characteristic (ROC) curve analysis [0.57 (95% confidence interval (CI) 0.51-0.61) and 0.6 (95% CI, 0.55-0.64), respectively], but high negative predictive values (NPV) [97.5% (95% CI 96.5-98.5) and 98.2% (95% CI 97.5-98.9) for PCT and CRP, respectively]. CRP alone was associated with bacterial coinfection (OR 2, 95% CI 1.25-3.19; p = 0.004). The overall 15, 30 and 90 days mortality had a higher trend in the bacterial coinfection group, but without significant difference. PCT ≥ 0.12 ng/mL was associated with higher 90 days mortality.
Our study suggests that measurements of PCT and CRP, alone and at a single time point, are not useful for ruling in or out bacterial coinfection in viral pneumonia by COVID-19.
虽然有报道称,在因 2019 年冠状病毒病(COVID-19)入院的患者中,社区获得性呼吸道细菌合并感染的患病率<5%,但几乎四分之三的患者接受了抗生素治疗。我们旨在研究降钙素原(PCT)或 C 反应蛋白(CRP)在入院时是否可作为有助于识别 COVID-19 肺炎患者细菌合并感染的生物标志物。
我们开展了一项多中心、观察性队列研究,纳入了 55 家西班牙重症监护病房(ICU)连续收治的 COVID-19 患者。主要结局是探讨 PCT 或 CRP 血清水平在入院时是否可预测 COVID-19 肺炎患者的细菌合并感染。次要结局是评估它们与死亡率的关系。我们还对高危人群进行了亚组分析。
2020 年 2 月 5 日至 2021 年 12 月 21 日,共纳入 4076 例患者,其中 133 例(3%)存在细菌合并感染。PCT 和 CRP 在受试者工作特征(ROC)曲线分析中的曲线下面积(AUC)评分较低[0.57(95%置信区间(CI)0.51-0.61)和 0.6(95%CI,0.55-0.64)],但阴性预测值(NPV)较高[分别为 97.5%(95%CI 96.5-98.5)和 98.2%(95%CI 97.5-98.9)]。CRP 单独与细菌合并感染相关(比值比 2,95%CI 1.25-3.19;p=0.004)。细菌合并感染组的总体 15、30 和 90 天死亡率呈上升趋势,但无统计学差异。PCT≥0.12ng/mL 与较高的 90 天死亡率相关。
本研究表明,PCT 和 CRP 单独或在单一时间点的测量值,不能用于确定 COVID-19 病毒性肺炎是否存在细菌合并感染。