Xu Zihui, Huang Anxiong, Luo Xun, Zhang Peng, Huang Lingli, Wang Xu, Mi Kun, Fang Shiwei, Huang Xiao, Li Jun, Yuan Zonghui, Hao Haihong
National Reference Laboratory of Veterinary Drug Residues (HZAU) and MAO Key Laboratory for Detection of Veterinary Drug Residues, Huazhong Agricultural University, Wuhan 430070, China.
MOA Laboratory for Risk Assessment of Quality and Safety of Livestock and Poultry Products, Huazhong Agricultural University, Wuhan 430070, China.
Antibiotics (Basel). 2021 Jul 2;10(7):808. doi: 10.3390/antibiotics10070808.
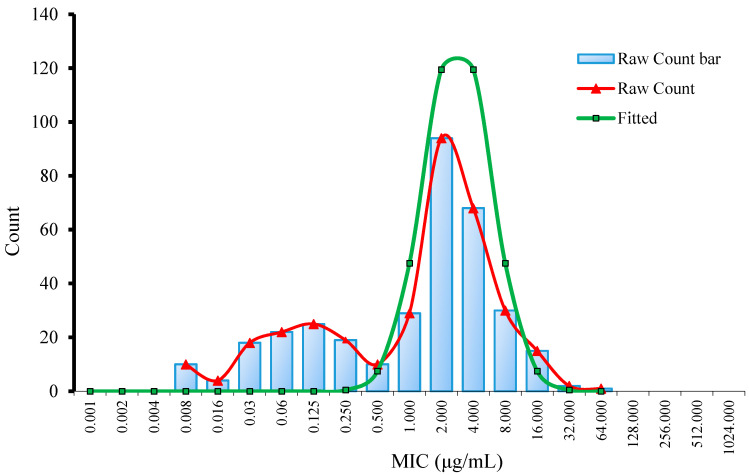
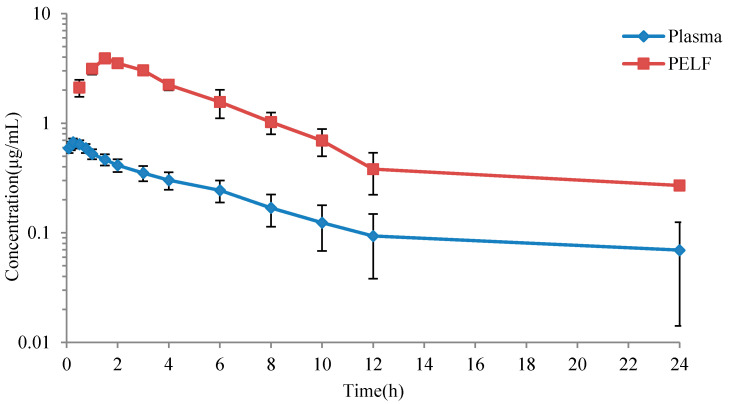
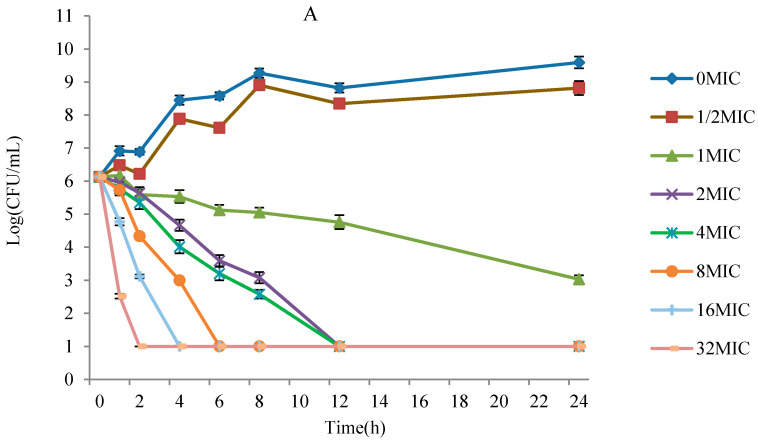
In order to establish the clinical breakpoint (CBP) of danofloxacin against , three cutoff values, including epidemiological cutoff value (ECV), pharmacokinetic-pharmacodynamic (PK-PD) cutoff value (CO) and clinical cutoff value (CO), were obtained in the present study. The ECV was calculated using ECOFFinder base on the MIC distribution of danfloxacin against 347 collected from disease pigs. The CO was established based on in vivo and ex vivo PK-PD modeling of danofloxacin both in plasma and pulmonary epithelial lining fluid (PELF) using Hill formula and Monte Carlo analysis. The CO was established based on the relationship between the possibility of cure (POC) and MIC in the clinical trials using the "WindoW" approach, nonlinear regression and CART analysis. The MIC and MIC of danofloxacin against 347 were 2 μg/mL and 8 μg/mL, respectively. The ECV value was set to 8 μg/mL using ECOFFinder. Concentration-time curves of danofloxacin were fitted with a two-compartment PK model. The PK parameters of the maximum concentration (C) and area under concentration-time curves (AUC) in PELF were 3.67 ± 0.25 μg/mL and 24.28 ± 2.70 h·μg/mL, higher than those in plasma (0.67 ± 0.01 μg/mL and 4.47 ± 0.51 h·μg/mL). The peak time (T) in plasma was 0.23 ± 0.07 h, shorter than that in PELF (1.61 ± 0.15 h). The CO in plasma and PELF were 0.125 μg/mL and 0.5 μg/mL, respectively. The CO calculated by WindoW approach, nonlinear regression and CART analysis were 0.125-4 μg/mL, 0.428 μg/mL and 0.56 μg/mL, respectively. The 0.5 μg/mL was selected as eligible CO. The ECV is much higher than the CO and CO, and the clinical breakpoint based on data in plasma was largely different from that of PELF. Our study firstly established three cutoff values of danofloxacin against It suggested that non-wild-type danofloxacin-resistant may lead to ineffective treatment by danofloxacin.
为确定达氟沙星对[具体病原菌名称未给出]的临床断点(CBP),本研究获得了三个截断值,包括流行病学截断值(ECV)、药代动力学 - 药效学(PK - PD)截断值(CO)和临床截断值(CO)。ECV是使用ECOFFinder根据从患病猪采集的347株[具体病原菌名称未给出]的达氟沙星MIC分布计算得出。CO是基于达氟沙星在血浆和肺上皮衬液(PELF)中的体内和体外PK - PD建模,使用希尔公式和蒙特卡罗分析确定的。CO是基于临床试验中治愈率(POC)与MIC之间的关系,采用“WindoW”方法、非线性回归和CART分析确定的。达氟沙星对347株[具体病原菌名称未给出]的MIC和MIC分别为2μg/mL和8μg/mL。使用ECOFFinder将ECV值设定为8μg/mL。达氟沙星的浓度 - 时间曲线用二室PK模型拟合。PELF中最大浓度(C)和浓度 - 时间曲线下面积(AUC)的PK参数分别为3.67±0.25μg/mL和24.28±2.70 h·μg/mL,高于血浆中的参数(0.67±0.01μg/mL和4.47±0.51 h·μg/mL)。血浆中的达峰时间(T)为0.23±0.07 h,短于PELF中的达峰时间(1.61±0.15 h)。血浆和PELF中的CO分别为0.125μg/mL和0.5μg/mL。通过“WindoW”方法、非线性回归和CART分析计算出的CO分别为0.125 - 4μg/mL、0.428μg/mL和0.56μg/mL。选择0.5μg/mL作为合适的CO。ECV远高于CO和CO,基于血浆数据的临床断点与PELF的临床断点有很大差异。我们的研究首次确定了达氟沙星对[具体病原菌名称未给出]的三个截断值。这表明非野生型达氟沙星耐药的[具体病原菌名称未给出]可能导致达氟沙星治疗无效。