Sobieraj Piotr, Siński Maciej, Lewandowski Jacek
Department of Internal Medicine, Hypertension and Vascular Diseases, Faculty of Medicine, Medical University of Warsaw, Banacha Str 1a, 02-097 Warsaw, Poland.
J Clin Med. 2021 Jul 24;10(15):3264. doi: 10.3390/jcm10153264.
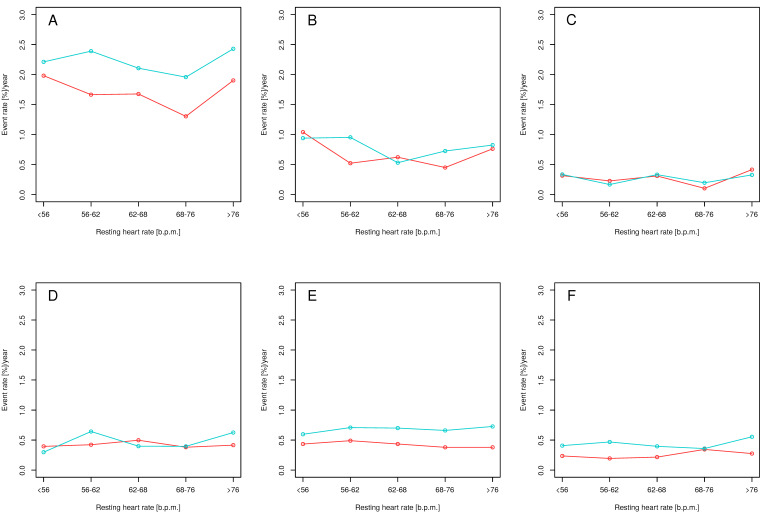
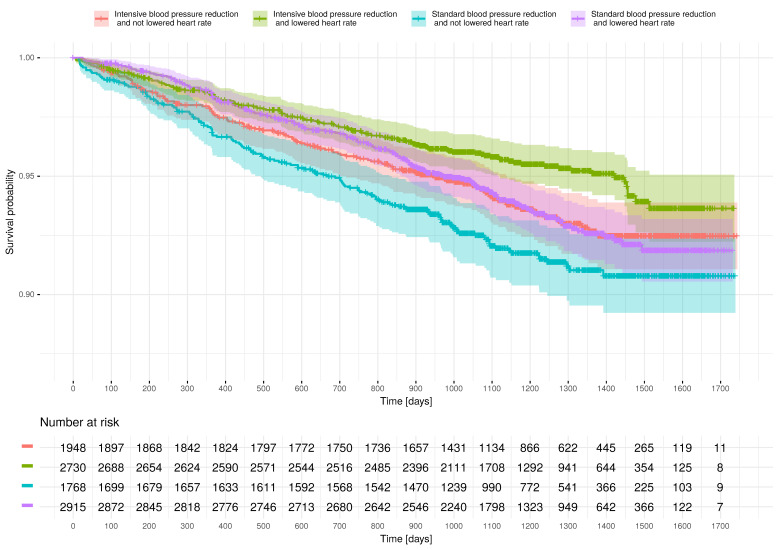
The association between elevated resting heart rate (RHR) as a cardiovascular risk factor and lowering of systolic blood pressure (SBP) to currently recommended values remain unknown. Systolic Blood Pressure Intervention Trial (SPRINT) data obtained from the NHLBI were used to describe the relationship between RHR and SBP reduction to <120 mmHg compared to SBP reduction to <140 mmHg. The composite clinical endpoint (CE) was defined as myocardial infarction, acute coronary syndrome, decompensation of heart failure, stroke, or cardiovascular death. Increased RHR was associated with a higher CE risk compared with low RHR in both treatment arms. A more potent increase of risk for CE was observed in subjects who were allocated to the SBP < 120 mmHg treatment goal. A similar effect of intensive and standard blood pressure (BP) reduction ( for interaction, 0.826) was observed in subjects with RHR in the 5th quintile (hazard ratio, 0.78, with 95% confidence interval (CI), 0.55-1.11) and in other quintiles of baseline RHR (hazard ratio, 0.75, with 95% CI, 0.62-0.90). Lower in-trial than baseline RHR was associated with reduced CE risk (hazard ratio, 0.80, with 95% CI, 0.66-0.98). We concluded that elevated RHR remains an essential risk factor independent of SBP reduction.
静息心率(RHR)升高作为心血管危险因素与将收缩压(SBP)降至当前推荐值之间的关联尚不清楚。利用从美国国立心肺血液研究所(NHLBI)获得的收缩压干预试验(SPRINT)数据来描述RHR与SBP降至<120 mmHg相比降至<140 mmHg之间的关系。复合临床终点(CE)定义为心肌梗死、急性冠状动脉综合征、心力衰竭失代偿、中风或心血管死亡。在两个治疗组中,与低RHR相比,RHR升高与更高的CE风险相关。在被分配到SBP<120 mmHg治疗目标的受试者中,观察到CE风险有更显著的增加。在RHR处于第5五分位数的受试者(风险比,0.78,95%置信区间(CI),0.55 - 1.11)和基线RHR的其他五分位数中(风险比,0.75,95% CI,0.62 - 0.90),观察到强化降压和标准血压(BP)降低有类似的效果(交互作用,0.826)。试验期间RHR低于基线与CE风险降低相关(风险比,0.80,95% CI,0.66 - 0.98)。我们得出结论,RHR升高仍然是一个独立于SBP降低的重要危险因素。