Department of Neurology, Danish Dementia Research Centre, Rigshospitalet, University of Copenhagen, Copenhagen, Denmark.
Alzheimer Center Amsterdam, Department of Neurology, Amsterdam Neuroscience, Vrije Universiteit Amsterdam, Amsterdam UMC, Amsterdam, the Netherlands.
J Alzheimers Dis. 2021;83(2):741-751. doi: 10.3233/JAD-210278.
Evidence-based recommendations on the optimal evaluation approach for dementia diagnostics are limited. This impedes a harmonized workup across clinics and nations.
To evaluate the diagnostic performance of a multidisciplinary consensus conference compared to a single clinician approach.
In this prospective study, we enrolled 457 patients with suspected cognitive decline, from two European memory clinics. A diagnostic evaluation was performed at baseline independently in two ways: 1) by a single clinician and 2) at a multidisciplinary consensus conference. A syndrome diagnosis and an etiological diagnosis was made. The confidence in the diagnosis was recorded using a visual analogue scale. An expert panel re-evaluation diagnosis served as reference for the baseline syndrome diagnosis and a 12-24-month follow-up diagnosis for the etiological diagnosis.
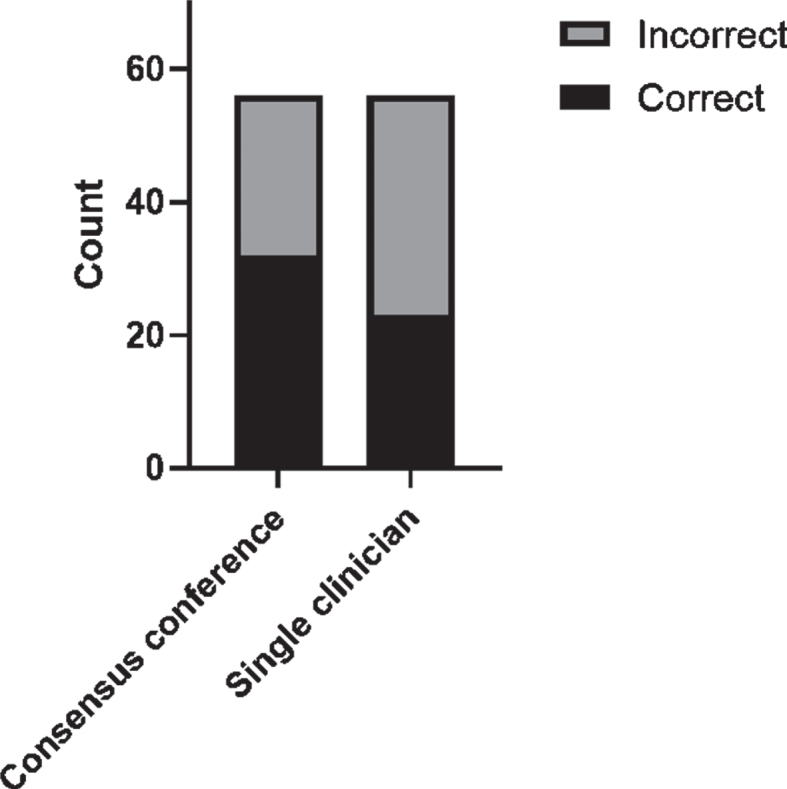
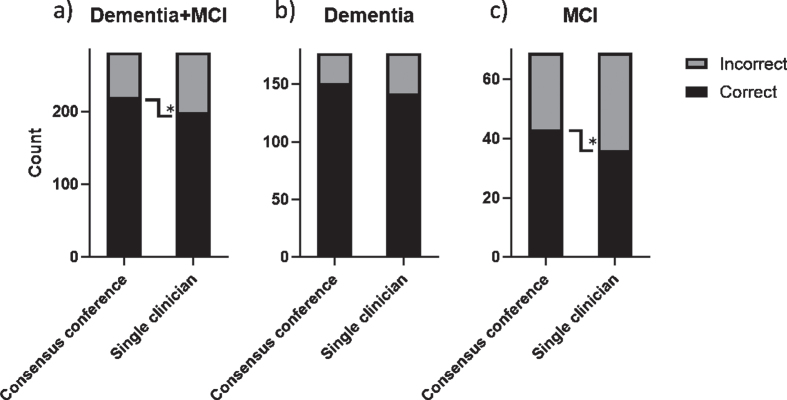
439 patients completed the study. We observed 12.5%discrepancy (k = 0.81) comparing the baseline syndrome diagnoses of the single clinician to the consensus conference, and 22.3%discrepancy (k = 0.68) for the baseline etiological diagnosis. The accuracy of the baseline etiological diagnosis was significantly higher at the consensus conference and was driven mainly by increased accuracy in the MCI group. Confidence in the etiological diagnosis at baseline was significantly higher at the consensus conference (p < 0.005), especially for the frontotemporal dementia diagnosis.
The multidisciplinary consensus conference performed better on diagnostic accuracy of disease etiology and increased clinicians' confidence. This highlights the importance of a multidisciplinary diagnostic evaluation approach for dementia diagnostics, especially when evaluating patients in the MCI stage.
目前针对痴呆症诊断的最佳评估方法,仅有有限的循证推荐,这阻碍了不同诊所和国家之间的协调评估。
评估多学科共识会议与单一临床医生方法在诊断性能上的差异。
在这项前瞻性研究中,我们纳入了来自两家欧洲记忆诊所的 457 名疑似认知能力下降的患者。在基线时,通过两种独立的方法进行诊断评估:1)由单一临床医生进行,2)在多学科共识会议上进行。做出综合征诊断和病因诊断,并使用视觉模拟量表记录诊断的信心程度。专家小组重新评估的诊断结果作为基线综合征诊断的参考,以及 12-24 个月的随访诊断作为病因诊断的参考。
439 名患者完成了研究。我们观察到,与共识会议相比,单一临床医生的基线综合征诊断存在 12.5%的差异(k=0.81),基线病因诊断存在 22.3%的差异(k=0.68)。共识会议上的基线病因诊断准确性明显更高,这主要归因于 MCI 组的准确性提高。共识会议上的基线病因诊断的信心明显更高(p<0.005),特别是在额颞叶痴呆的诊断上。
多学科共识会议在疾病病因的诊断准确性和提高临床医生信心方面表现更好。这突出了多学科诊断评估方法在痴呆症诊断中的重要性,特别是在评估 MCI 阶段的患者时。