Hartley Adam, El-Sayed Ahmed, Abbara Aula, Henderson Jamie, Ghazy Anan, Davies Frances, Price James R, Punjabi Prakash P, Anderson Jon, Casula Roberto, Naderi Hafiz, Asaria Perviz, Sutaria Nilesh, Malik Iqbal S, Pabari Punam A, Rana Bushra S
National Heart and Lung Institute, Imperial College London, London, UK.
Imperial College Healthcare NHS Trust, London, UK.
Cardiol Res Pract. 2021 Jul 30;2021:5565200. doi: 10.1155/2021/5565200. eCollection 2021.
Infective endocarditis (IE) is challenging to manage in the COVID-19 lockdown period, in part given its reliance on echocardiography for diagnosis and management and the associated virus transmission risks to patients and healthcare workers. This study assesses utilisation of the endocarditis team (ET) in limiting routine echocardiography, especially transoesophageal echocardiography (TOE), in patients with suspected IE, and explores the effect on clinical outcomes.
All patients discussed at the ET meeting at Imperial College Healthcare NHS Trust during the first lockdown in the UK (23 March to 8 July 2020) were prospectively included and analysed in this observational study.
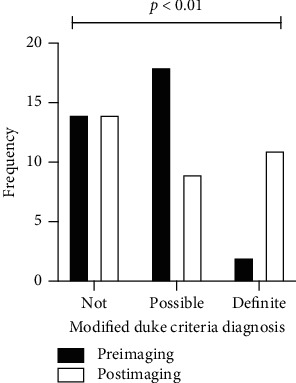
In total, 38 patients were referred for ET review (71% male, median age 54 [interquartile range 48, 65.5] years). At the time of ET discussion, 21% had no echo imaging, 16% had point-of-care ultrasound only, and 63% had formal TTE. In total, only 16% underwent TOE. The ability of echocardiography, in those where it was performed, to affect IE diagnosis according to the Modified Duke Criteria was significant (=0.0099); however, sensitivity was not affected. All-cause mortality was 17% at 30 days and 25% at 12 months from ET discussion in those with confirmed IE.
Limiting echocardiography in patients with a low pretest probability (not probable or definite IE according to the Modified Duke Criteria) did not affect the diagnostic ability of the Modified Duke Criteria to rule out IE in this small study. Moreover, restricting nonessential echocardiography, and importantly TOE, in patients with suspected IE through use of the ET did not impact all-cause mortality.
在新冠疫情封锁期间,感染性心内膜炎(IE)的管理颇具挑战,部分原因在于其诊断和管理依赖超声心动图,且存在病毒传播给患者和医护人员的风险。本研究评估了心内膜炎团队(ET)在限制疑似IE患者的常规超声心动图检查,尤其是经食管超声心动图(TOE)检查方面的应用情况,并探讨其对临床结局的影响。
在英国首次封锁期间(2020年3月23日至7月8日),前瞻性纳入并分析了在帝国理工学院医疗保健国民信托基金ET会议上讨论的所有患者。
共有38例患者被转诊至ET进行评估(71%为男性,中位年龄54岁[四分位间距48, 65.5岁])。在ET讨论时,21%的患者未进行超声心动图检查,16%的患者仅进行了床旁超声检查,63%的患者进行了正式的经胸超声心动图(TTE)检查。总共只有16%的患者接受了TOE检查。根据改良杜克标准,超声心动图检查对IE诊断的影响具有显著性(P = 0.0099);然而,敏感性未受影响。确诊IE患者自ET讨论起30天的全因死亡率为17%,12个月时为25%。
在这项小型研究中,对于预检概率较低(根据改良杜克标准不太可能或肯定不是IE)的患者限制超声心动图检查,并未影响改良杜克标准排除IE的诊断能力。此外,通过ET对疑似IE患者限制非必要的超声心动图检查,尤其是TOE检查,并未影响全因死亡率。