Department of Anesthesiology and Intensive Care Medicine, Universitätsklinikum Leipzig, Leipzig, Sachsen, Germany.
Department of Anesthesiology, Intensive Care, and Emergency Medicine, BG Klinikum Bergmannstrost Halle, Halle, Sachsen-Anhalt, Germany.
Emerg Med J. 2022 Jul;39(7):534-539. doi: 10.1136/emermed-2021-211786. Epub 2021 Aug 10.
Emergency tracheal intubation during major trauma resuscitation may be associated with unrecognised endobronchial intubation. The risk factors and outcomes associated with this issue have not previously been fully defined.
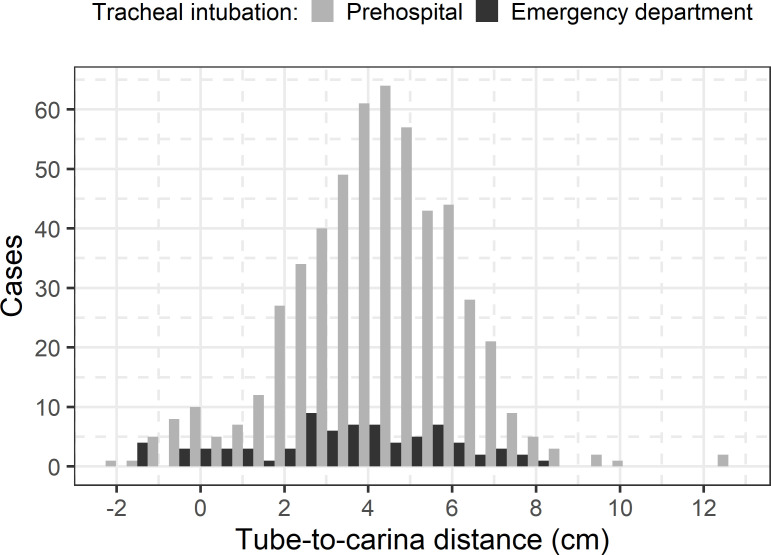
We retrospectively analysed adult patients admitted directly from the scene to the ED of a single level 1 trauma centre, who received either prehospital or ED tracheal intubation prior to initial whole-body CT from January 2008 to December 2019. Our objectives were to describe tube-to-carina distances (TCDs) via CT and to assess the risk factors and outcomes (mortality, length of intensive care unit stay and mechanical ventilation) of patients with endobronchial intubation (TCD <0 cm) using a multivariable model.
We included 616 patients and discovered 26 (4.2%) cases of endobronchial intubation identified on CT. Factors associated with an increased risk of endobronchial intubations were short body height (OR per 1 cm increase 0.89; 95% CI 0.84 to 0.94; p≤0.001), a high body mass index (OR 1.14; 95% CI 1.04 to 1.25; p=0.005) and ED intubation (OR 3.62; 95% CI 1.39 to 8.90; p=0.006). Eight of 26 cases underwent tube thoracostomy, four of whom had no evidence of underlying chest injury on CT. There was no statistically significant difference in mortality or length of stay although the absolute number of endobronchial intubations was small.
Short body height and high body mass index were associated with endobronchial intubation. Before considering tube thoracostomy in intubated major trauma patients suspected of pneumothorax, the possibility of unrecognised endobronchial intubation should be considered.
在严重创伤复苏期间进行紧急气管插管可能与未被识别的支气管内插管有关。先前并未完全明确与这一问题相关的危险因素和结局。
我们回顾性分析了 2008 年 1 月至 2019 年 12 月期间,直接从现场收入一家一级创伤中心急诊室的成年患者,这些患者在接受初始全身 CT 之前,曾接受过院前或急诊室气管插管。我们的目的是描述 CT 下的气管隆嵴距离(TCD),并使用多变量模型评估支气管内插管(TCD<0cm)患者的危险因素和结局(死亡率、重症监护病房住院时间和机械通气)。
我们纳入了 616 例患者,发现 26 例(4.2%)患者在 CT 上存在支气管内插管。与支气管内插管风险增加相关的因素包括:身高较矮(每增加 1cm,比值比 0.89;95%置信区间 0.84 至 0.94;p≤0.001)、高体重指数(比值比 1.14;95%置信区间 1.04 至 1.25;p=0.005)和急诊室插管(比值比 3.62;95%置信区间 1.39 至 8.90;p=0.006)。26 例中 8 例行胸腔管引流术,其中 4 例 CT 未见明显胸部损伤。尽管支气管内插管的绝对数量较少,但死亡率或住院时间无统计学差异。
身高较矮和高体重指数与支气管内插管有关。在考虑对怀疑气胸的插管严重创伤患者进行胸腔管引流术之前,应考虑到未被识别的支气管内插管的可能性。