Global and Tropical Health Division, Menzies School of Health Research, Charles Darwin University, Australia (J.R.F., H.F., J.M., J.Y., A.P.R., B.R.).
Department of Pediatrics, Royal Darwin Hospital, Australia (J.R.F., H.H., A.H., L.A.F., K.D., J.Y., K.V.R., B.R.).
Circ Cardiovasc Imaging. 2021 Aug;14(8):e011790. doi: 10.1161/CIRCIMAGING.120.011790. Epub 2021 Aug 13.
Echocardiographic screening can detect asymptomatic cases of rheumatic heart disease (RHD), facilitating access to treatment. Barriers to implementation of echocardiographic screening include the requirement for expensive equipment and expert practitioners. We aimed to evaluate the diagnostic accuracy of an abbreviated echocardiographic screening protocol (single parasternal-long-axis view with a sweep of the heart) performed by briefly trained, nonexpert practitioners using handheld ultrasound devices.
Participants aged 5 to 20 years in Timor-Leste and the Northern Territory of Australia had 2 echocardiograms: one performed by an expert echocardiographer using a GE Vivid I or Vivid Q portable ultrasound device (reference test), and one performed by a nonexpert practitioner using a GE Vscan handheld ultrasound device (index test). The accuracy of the index test, compared with the reference test, for identifying cases with definite or borderline RHD was determined.
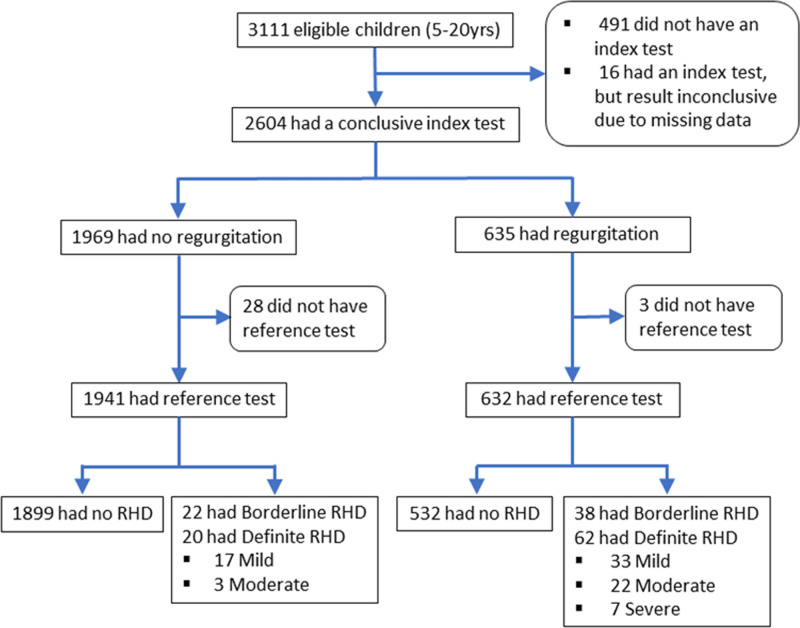
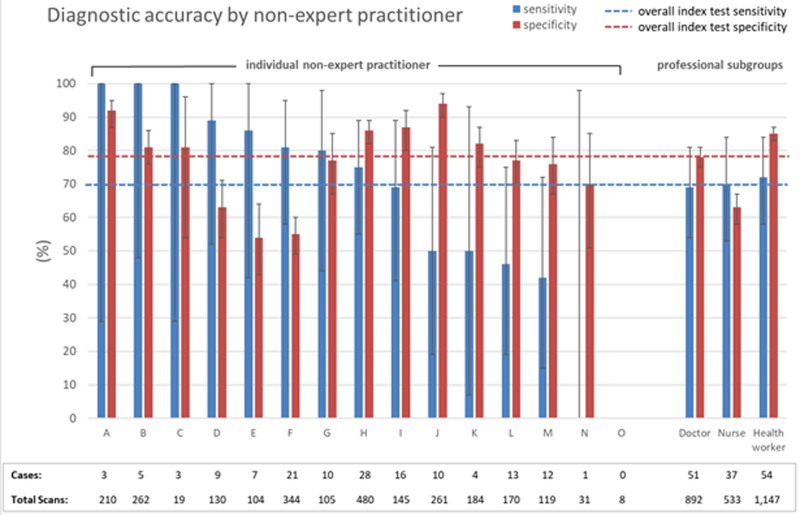
There were 3111 enrolled participants; 2573 had both an index test and reference test. Median age was 12 years (interquartile range, 10-15); 58.2% were female. Proportion with definite or borderline RHD was 5.52% (95% CI, 4.70-6.47); proportion with definite RHD was 3.23% (95% CI, 2.61-3.98). Compared with the reference test, sensitivity of the index test for definite or borderline RHD was 70.4% (95% CI, 62.2-77.8), specificity was 78.1% (95% CI, 76.4-79.8).
Nonexpert practitioners can be trained to perform single parasternal-long-axis view with a sweep of the heart echocardiography. However, the specificity and sensitivity are inadequate for echocardiographic screening. Improved training for nonexpert practitioners should be investigated.
超声心动图筛查可发现无症状性风湿性心脏病(RHD)病例,从而便于治疗。实施超声心动图筛查的障碍包括需要昂贵的设备和专业医生。我们旨在评估由经过短期培训的非专业医生使用手持式超声设备进行简化超声心动图筛查方案(单一胸骨旁长轴切面加心脏扫查)的诊断准确性。
东帝汶和澳大利亚北部地区年龄在 5 岁至 20 岁的参与者接受了 2 次超声心动图检查:一次由专家使用 GE Vivid I 或 Vivid Q 便携式超声设备(参考测试)进行,一次由非专业医生使用 GE Vscan 手持式超声设备(指标测试)进行。通过参考测试确定了指标测试对确定或临界 RHD 病例的准确性。
共纳入 3111 名参与者;其中 2573 名参与者进行了指数测试和参考测试。中位年龄为 12 岁(四分位距,10-15);58.2%为女性。确定或临界 RHD 的比例为 5.52%(95%CI,4.70-6.47);确定 RHD 的比例为 3.23%(95%CI,2.61-3.98)。与参考测试相比,指标测试对确定或临界 RHD 的敏感性为 70.4%(95%CI,62.2-77.8),特异性为 78.1%(95%CI,76.4-79.8)。
可以培训非专业医生进行单一胸骨旁长轴切面加心脏扫查的超声心动图检查。但是,特异性和敏感性不足以进行超声心动图筛查。应该研究对非专业医生的改进培训。