Fradley Michael G, Ellenberg Kerry, Alomar Mohammed, Swanson Justin, Kharod Anant, Nguyen Anh Thy H, Khodor Sara, Mishra Shreya, Duong Linh M, Shah Nirav, Armanious Merna, Rhea Isaac B, Schabath Matthew B, Kip Kevin E
Cardio-Oncology Center of Excellence, Division of Cardiology, Department of Medicine, Perelman School of Medicine at the University of Pennsylvania, Philadelphia, Pennsylvania, USA.
Cardio-Oncology Program, H. Lee Moffitt Cancer Center and Research Institute and University of South Florida Morsani College of Medicine, Tampa, Florida, USA.
JACC CardioOncol. 2020 Dec 15;2(5):747-754. doi: 10.1016/j.jaccao.2020.09.008. eCollection 2020 Dec.
Atrial fibrillation (AF) is a common cardiovascular complication affecting patients with cancer, but management strategies are not well established.
The purpose of this retrospective cohort study was to evaluate cross-sectional patterns of anticoagulation (AC) use in patients with cancer with AF or atrial flutter (AFL) on the basis of their risk for stroke and bleeding.
Patients with cancer and electrocardiograms showing AF or AFL performed at Moffitt Cancer Center in either the inpatient or outpatient setting were included in this retrospective analysis. We described percentages of AC prescription by stroke and bleeding risk, as determined by individual CHADS-VASc and HAS-BLED scores, respectively. Multivariable logistic regression evaluated clinical variables independently associated with anticoagulant prescription.
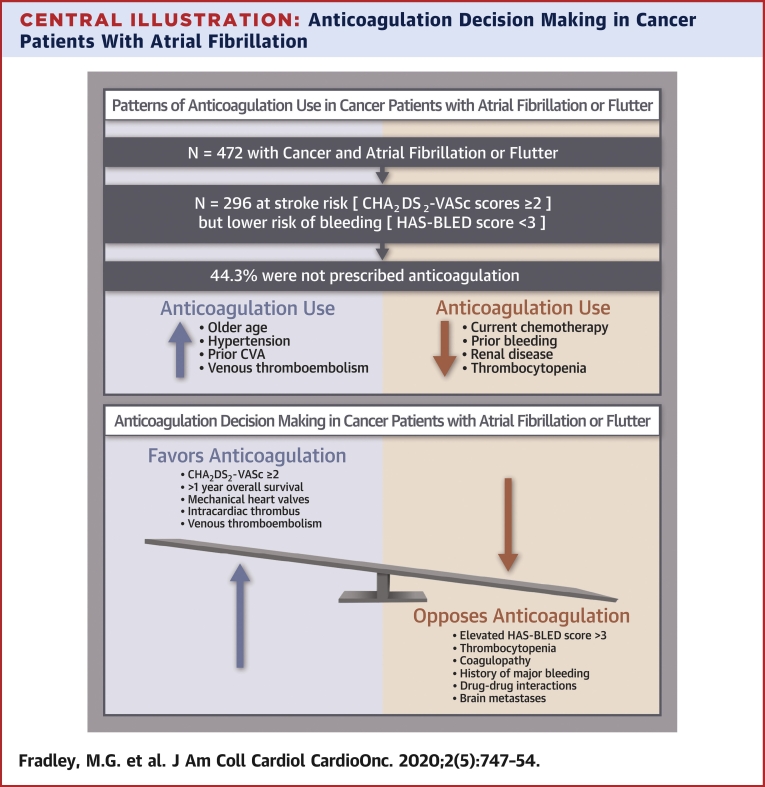
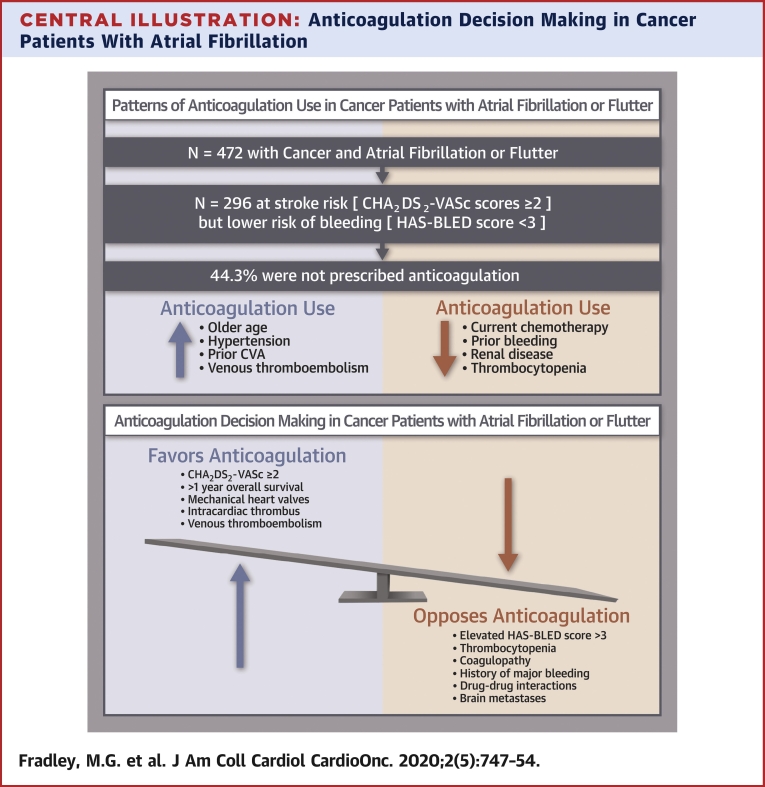
The prevalence of electrocardiography-documented AF or AFL was 4.8% (n = 472). The mean CHADS-VASc score was 2.8 ± 1.4. Among patients with CHADS-VASc scores ≥2 and HAS-BLED scores <3, 44.3% did not receive AC, and of these, only 18.3% had platelet values <50,000/μl. In multivariable analysis, older age, hypertension, prior stroke, and history of venous thromboembolism were each directly associated with AC use, while current chemotherapy use, prior bleeding, renal disease, and thrombocytopenia were each inversely associated with AC use.
Nearly one-half of patients with cancer, the majority with normal platelet counts, had an elevated risk for stroke but did not receive AC. In addition to known predictors, current chemotherapy use was independently associated with a lower odds of AC use. This study highlights the need to improve the application of AF treatment algorithms to cancer populations.
心房颤动(AF)是影响癌症患者的常见心血管并发症,但管理策略尚未完全确立。
这项回顾性队列研究的目的是根据癌症合并房颤或房扑(AFL)患者的卒中风险和出血风险,评估抗凝(AC)治疗的横断面使用模式。
本回顾性分析纳入了在莫菲特癌症中心住院或门诊进行心电图检查显示为房颤或房扑的癌症患者。我们分别根据个体CHADS-VASc和HAS-BLED评分确定的卒中风险和出血风险描述了AC处方的百分比。多变量逻辑回归评估了与抗凝处方独立相关的临床变量。
心电图记录的房颤或房扑患病率为4.8%(n = 472)。CHADS-VASc评分的平均值为2.8±1.4。在CHADS-VASc评分≥2且HAS-BLED评分<3的患者中,44.3%未接受AC治疗,其中只有18.3%的血小板值<50,000/μl。在多变量分析中,年龄较大、高血压、既往卒中以及静脉血栓栓塞病史均与AC治疗直接相关,而当前使用化疗、既往出血、肾脏疾病和血小板减少症均与AC治疗呈负相关。
近一半的癌症患者,大多数血小板计数正常,卒中风险升高但未接受AC治疗。除了已知的预测因素外,当前使用化疗与AC治疗的较低几率独立相关。本研究强调了改进房颤治疗算法在癌症人群中应用的必要性。