Schlam Ilana, Lee Andy Y, Li Song, Sheikh Farooq H, Zaghlol Raja, Basyal Binaya, Gallagher Christopher, Molina Ezequiel, Mahr Claudius, Cheng Richard K, Barac Ana
MedStar Washington Cancer Institute, Washington, DC, USA.
Department of Hematology-Oncology, MedStar Washington Hospital Center, Washington, DC, USA.
JACC CardioOncol. 2021 Jun 15;3(2):305-315. doi: 10.1016/j.jaccao.2021.04.008. eCollection 2021 Jun.
There are limited data to guide oncology and cardiology decision-making in patients with a left ventricular assist device (LVAD) and concurrent active malignancy.
The goal of this study was to describe cancer treatment approaches, complications, and survival among patients with active cancer on LVAD support in 2 tertiary heart failure and oncology programs.
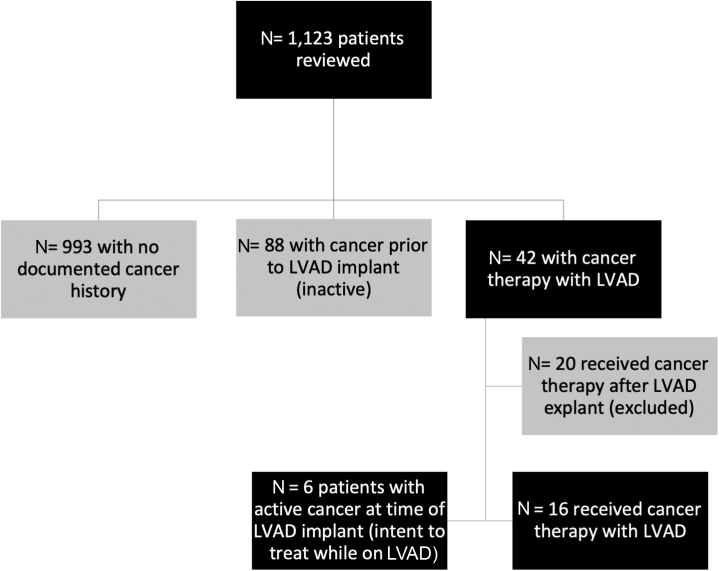
In this retrospective cohort study, LVAD databases were reviewed to identify patients with a cancer diagnosis at the time of or after LVAD implantation. We created a 3:1 matched cohort based on age, sex, etiology of cardiomyopathy, LVAD implant strategy, and INTERMACS profile stratified by site. Kaplan-Meier analysis and Cox proportional hazards models were used to compare survival between patients with cancer and non-cancer comparators.
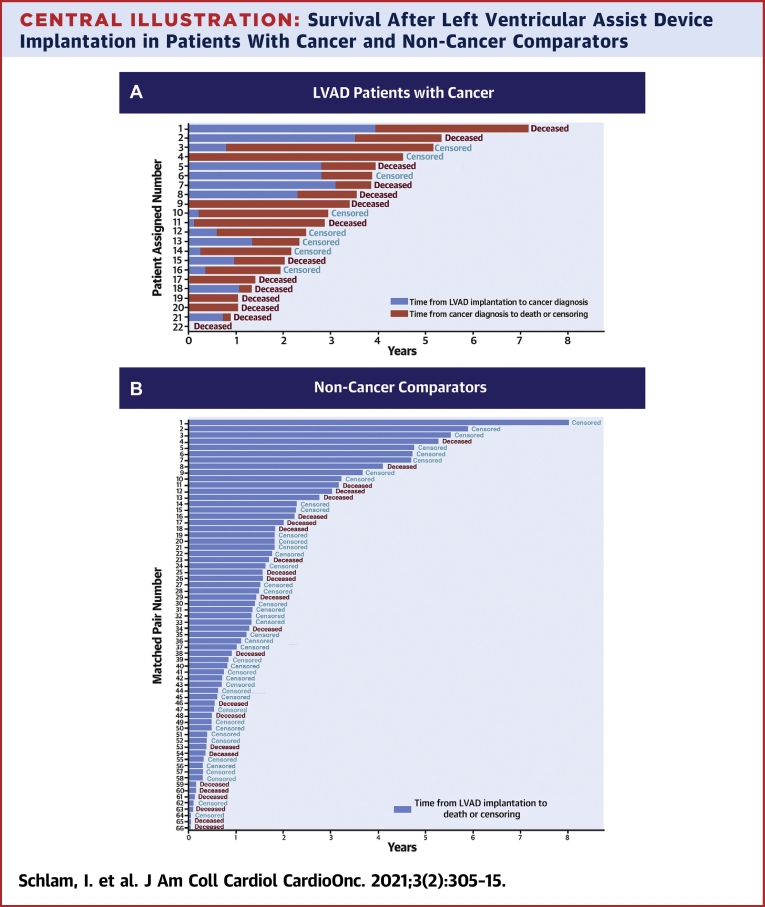
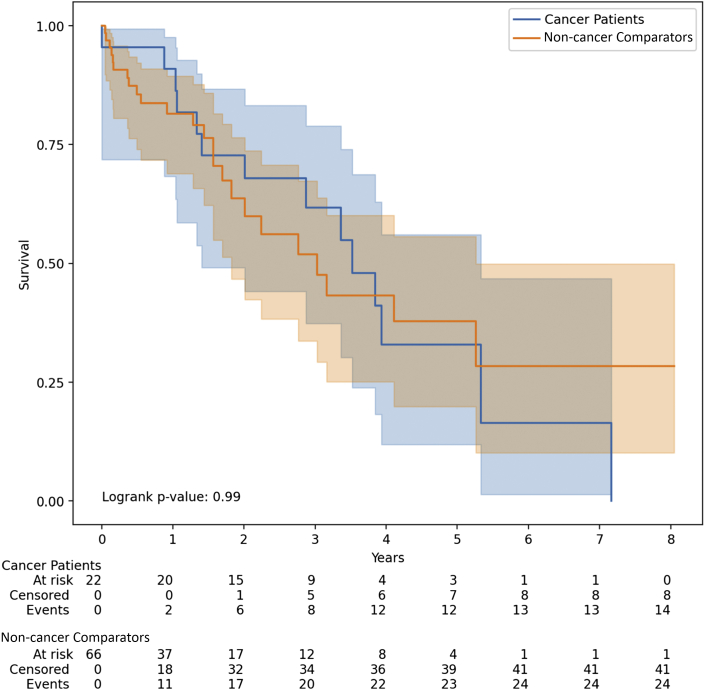
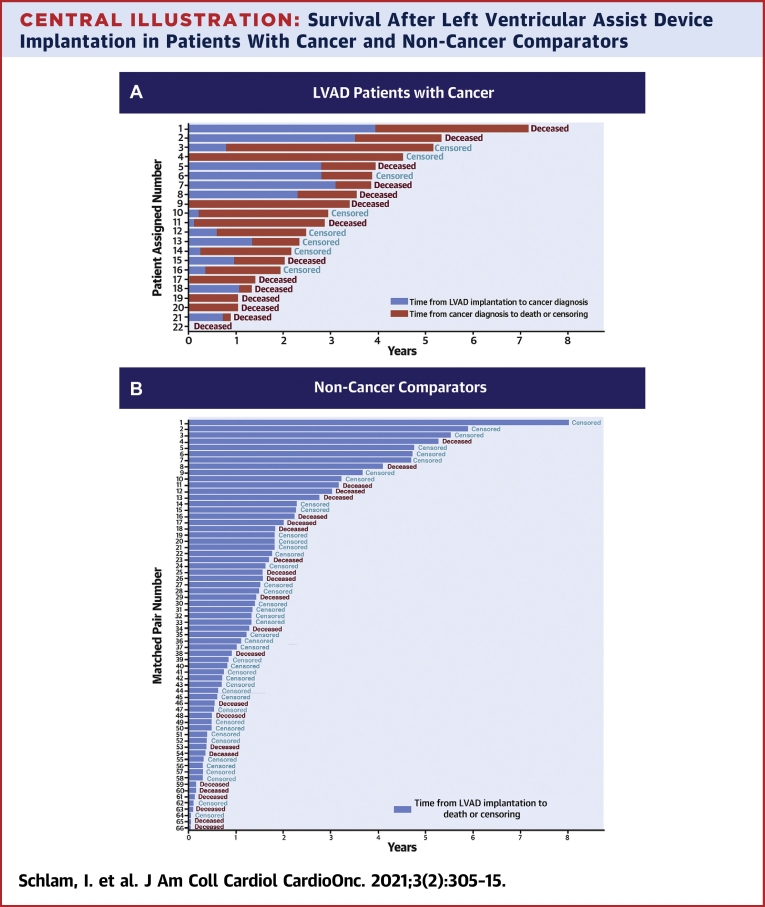
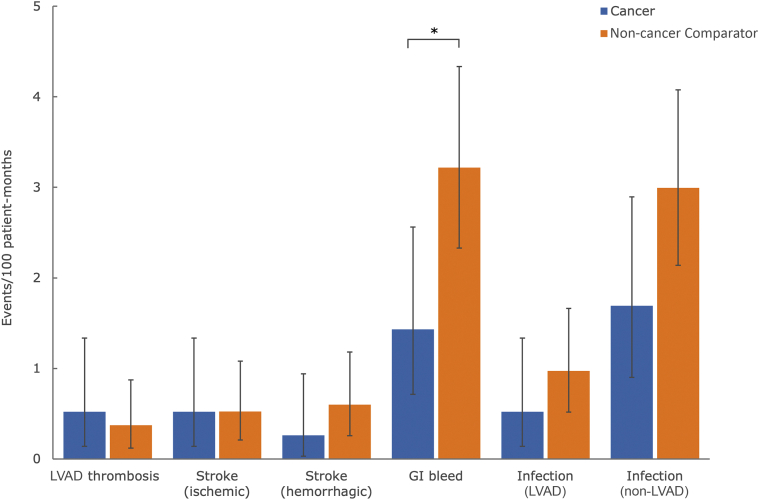
Among 1,123 patients who underwent LVAD implantation between 2005 and 2019, 22 patients with LVADs with active cancer and 66 matched non-cancer comparators were identified. Median age was 62 years (range 41 to 73 years); 50% of patients with cancer were African-American, and 27% were women. Prostate cancer, followed by renal cell cancer and hematologic malignancies were the most common diagnoses. There was no significant difference in unadjusted Kaplan-Meier median survival estimates from the time of LVAD placement between patients with cancer (3.53 years; 95% confidence interval [CI]: 1.41 to 5.33) and non-cancer comparators (3.03 years; 95% CI: 1.83 to 5.26; log-rank = 0.99). In Cox proportional hazard models, cancer diagnosis as a time-varying variable was associated with a statistically significant increase in death (hazard ratio: 2.05; 95% CI: 1.03 to 4.12; = 0.04). Patients with cancer had less gastrointestinal bleeding compared with matched non-cancer comparators ( = 0.016). Other complications were not significantly different.
Our study provides initial feasibility and safety data and set a framework for multidisciplinary team management of patients with cancer and LVADs.
在左心室辅助装置(LVAD)植入且同时患有活动性恶性肿瘤的患者中,用于指导肿瘤学和心脏病学决策的数据有限。
本研究的目的是描述在两个三级心力衰竭和肿瘤项目中接受LVAD支持的活动性癌症患者的癌症治疗方法、并发症和生存率。
在这项回顾性队列研究中,对LVAD数据库进行了回顾,以确定在LVAD植入时或植入后被诊断患有癌症的患者。我们根据年龄、性别、心肌病病因、LVAD植入策略以及按部位分层的INTERMACS概况创建了一个3:1匹配队列。采用Kaplan-Meier分析和Cox比例风险模型比较癌症患者与非癌症对照者的生存率。
在2005年至2019年间接受LVAD植入的1123例患者中,确定了22例患有活动性癌症的LVAD患者和66例匹配的非癌症对照者。中位年龄为62岁(范围41至73岁);50%的癌症患者为非裔美国人,27%为女性。前列腺癌、其次是肾细胞癌和血液系统恶性肿瘤是最常见的诊断。癌症患者(3.53年;95%置信区间[CI]:1.41至5.33)与非癌症对照者(3.03年;95%CI:1.83至5.26;对数秩=0.99)从LVAD植入时起的未调整Kaplan-Meier中位生存估计值无显著差异。在Cox比例风险模型中,将癌症诊断作为一个随时间变化的变量与死亡的统计学显著增加相关(风险比:2.05;95%CI:1.03至4.12;P=0.04)。与匹配的非癌症对照者相比,癌症患者的胃肠道出血较少(P=0.016)。其他并发症无显著差异。
我们的研究提供了初步的可行性和安全性数据,并为癌症患者和LVAD患者的多学科团队管理建立了一个框架。