Kyo Michihito, Shimatani Tatsutoshi, Hosokawa Koji, Taito Shunsuke, Kataoka Yuki, Ohshimo Shinichiro, Shime Nobuaki
Department of Emergency and Critical Care Medicine, Graduate School of Biomedical and Health Sciences, Hiroshima University, Kasumi 1-2-3, Minami-ku, Hiroshima, 734-8551, Japan.
Department of Anesthesiology and Reanimatology, Faculty of Medicine Sciences, University of Fukui, 23-3 Eiheijicho, Yoshidagun, Fukui, 910-1193, Japan.
J Intensive Care. 2021 Aug 16;9(1):50. doi: 10.1186/s40560-021-00565-5.
Patient-ventilator asynchrony (PVA) is a common problem in patients undergoing invasive mechanical ventilation (MV) in the intensive care unit (ICU), and may accelerate lung injury and diaphragm mis-contraction. The impact of PVA on clinical outcomes has not been systematically evaluated. Effective interventions (except for closed-loop ventilation) for reducing PVA are not well established.
We performed a systematic review and meta-analysis to investigate the impact of PVA on clinical outcomes in patients undergoing MV (Part A) and the effectiveness of interventions for patients undergoing MV except for closed-loop ventilation (Part B). We searched the Cochrane Central Register of Controlled Trials, MEDLINE, EMBASE, ClinicalTrials.gov, and WHO-ICTRP until August 2020. In Part A, we defined asynchrony index (AI) ≥ 10 or ineffective triggering index (ITI) ≥ 10 as high PVA. We compared patients having high PVA with those having low PVA.
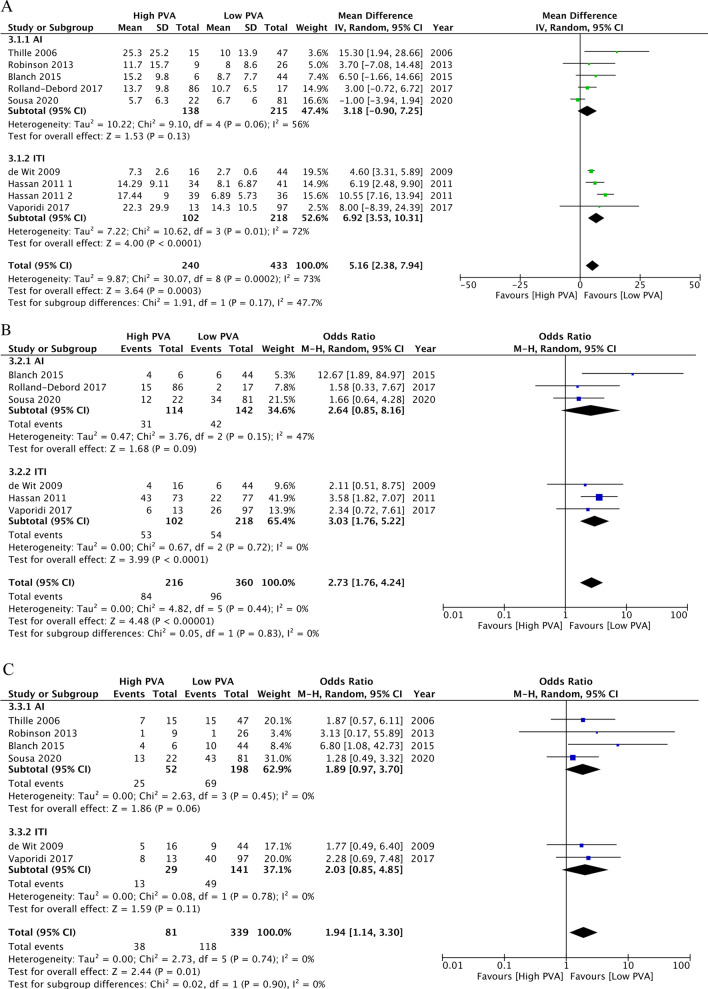
Eight studies in Part A and eight trials in Part B fulfilled the eligibility criteria. In Part A, five studies were related to the AI and three studies were related to the ITI. High PVA may be associated with longer duration of mechanical ventilation (mean difference, 5.16 days; 95% confidence interval [CI], 2.38 to 7.94; n = 8; certainty of evidence [CoE], low), higher ICU mortality (odds ratio [OR], 2.73; 95% CI 1.76 to 4.24; n = 6; CoE, low), and higher hospital mortality (OR, 1.94; 95% CI 1.14 to 3.30; n = 5; CoE, low). In Part B, interventions involving MV mode, tidal volume, and pressure-support level were associated with reduced PVA. Sedation protocol, sedation depth, and sedation with dexmedetomidine rather than propofol were also associated with reduced PVA.
PVA may be associated with longer MV duration, higher ICU mortality, and higher hospital mortality. Physicians may consider monitoring PVA and adjusting ventilator settings and sedatives to reduce PVA. Further studies with adjustment for confounding factors are warranted to determine the impact of PVA on clinical outcomes. Trial registration protocols.io (URL: https://www.protocols.io/view/the-impact-of-patient-ventilator-asynchrony-in-adu-bsqtndwn , 08/27/2020).
患者 - 呼吸机不同步(PVA)是重症监护病房(ICU)中接受有创机械通气(MV)患者的常见问题,可能会加速肺损伤和膈肌误收缩。PVA对临床结局的影响尚未得到系统评估。降低PVA的有效干预措施(闭环通气除外)尚未明确。
我们进行了一项系统评价和荟萃分析,以研究PVA对接受MV患者临床结局的影响(A部分)以及除闭环通气外接受MV患者干预措施的有效性(B部分)。我们检索了Cochrane对照试验中央注册库、MEDLINE、EMBASE、ClinicalTrials.gov和世界卫生组织国际临床试验注册平台,检索截至2020年8月。在A部分,我们将异步指数(AI)≥10或无效触发指数(ITI)≥10定义为高PVA。我们比较了高PVA患者和低PVA患者。
A部分的八项研究和B部分的八项试验符合纳入标准。在A部分,五项研究与AI相关,三项研究与ITI相关。高PVA可能与机械通气时间延长有关(平均差,5.16天;95%置信区间[CI],2.38至7.94;n = 8;证据确定性[CoE],低)、ICU死亡率较高(比值比[OR],2.73;95% CI 1.76至4.24;n = 6;CoE,低)以及医院死亡率较高(OR,1.94;95% CI 1.14至3.30;n = 5;CoE,低)。在B部分,涉及MV模式、潮气量和压力支持水平的干预措施与PVA降低有关。镇静方案、镇静深度以及使用右美托咪定而非丙泊酚镇静也与PVA降低有关。
PVA可能与MV时间延长、ICU死亡率较高和医院死亡率较高有关。医生可考虑监测PVA并调整呼吸机设置和镇静剂以降低PVA。有必要进行进一步调整混杂因素的研究,以确定PVA对临床结局的影响。试验注册 protocols.io(网址:https://www.protocols.io/view/the-impact-of-patient-ventilator-asynchrony-in-adu-bsqtndwn,2020年8月27日)。