Mishra Swapnil, Mindermann Sören, Sharma Mrinank, Whittaker Charles, Mellan Thomas A, Wilton Thomas, Klapsa Dimitra, Mate Ryan, Fritzsche Martin, Zambon Maria, Ahuja Janvi, Howes Adam, Miscouridou Xenia, Nason Guy P, Ratmann Oliver, Semenova Elizaveta, Leech Gavin, Sandkühler Julia Fabienne, Rogers-Smith Charlie, Vollmer Michaela, Unwin H Juliette T, Gal Yarin, Chand Meera, Gandy Axel, Martin Javier, Volz Erik, Ferguson Neil M, Bhatt Samir, Brauner Jan M, Flaxman Seth
Medical Research Council (MRC) Centre for Global Infectious Disease Analysis, Jameel Institute, School of Public Health, Imperial College London, UK.
Oxford Applied and Theoretical Machine Learning (OATML) Group, Department of Computer Science, University of Oxford, UK.
EClinicalMedicine. 2021 Jul 31;39:101064. doi: 10.1016/j.eclinm.2021.101064. eCollection 2021 Sep.
Since its emergence in Autumn 2020, the SARS-CoV-2 Variant of Concern (VOC) B.1.1.7 (WHO label Alpha) rapidly became the dominant lineage across much of Europe. Simultaneously, several other VOCs were identified globally. Unlike B.1.1.7, some of these VOCs possess mutations thought to confer partial immune escape. Understanding when and how these additional VOCs pose a threat in settings where B.1.1.7 is currently dominant is vital.
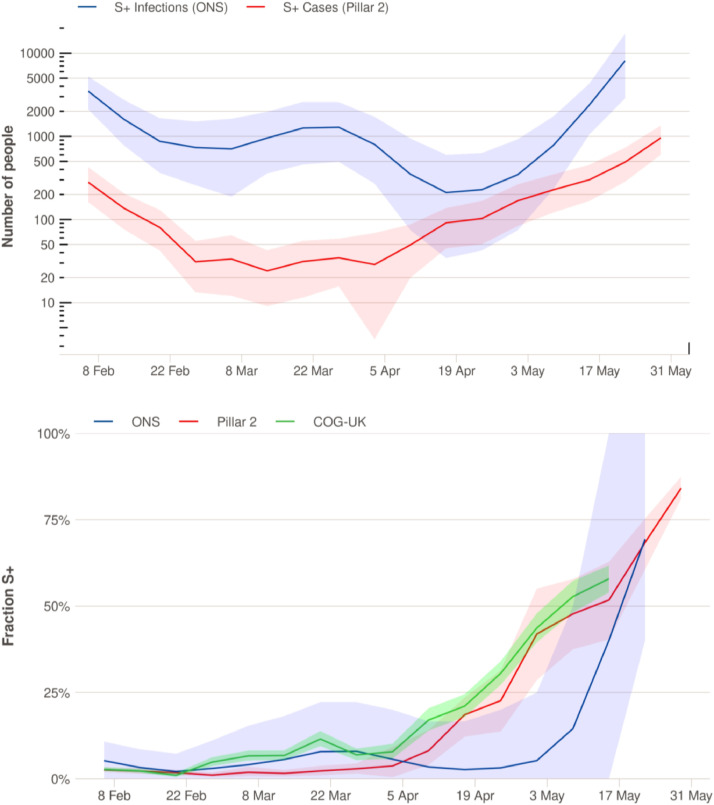
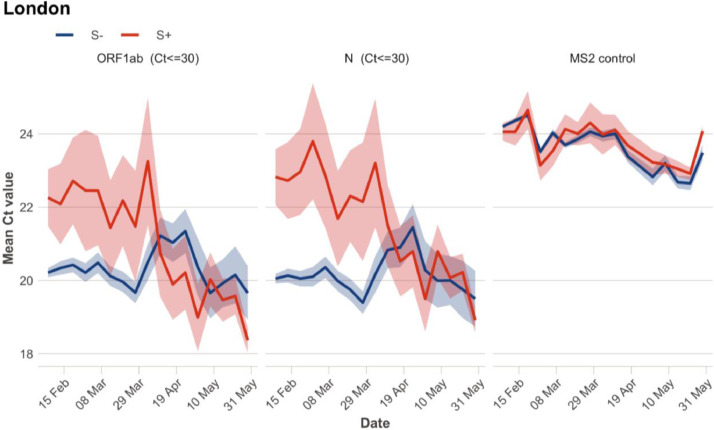
We examine trends in the prevalence of non-B.1.1.7 lineages in London and other English regions using passive-case detection PCR data, cross-sectional community infection surveys, genomic surveillance, and wastewater monitoring. The study period spans from 31st January 2021 to 15th May 2021.
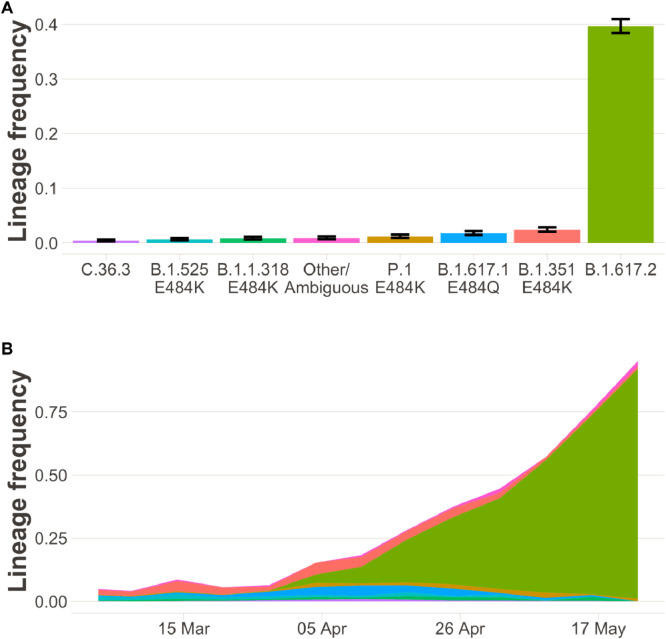
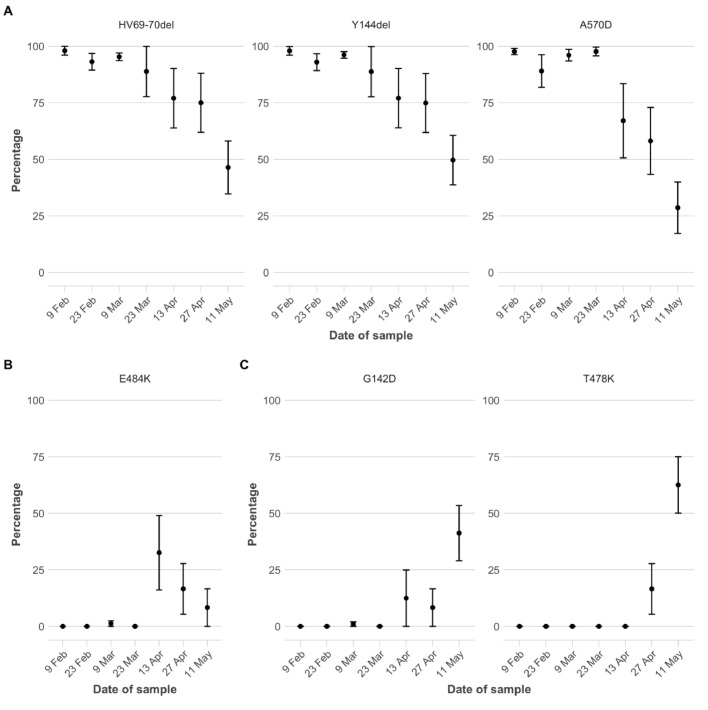
Across data sources, the percentage of non-B.1.1.7 variants has been increasing since late March 2021. This increase was initially driven by a variety of lineages with immune escape. From mid-April, B.1.617.2 (WHO label Delta) spread rapidly, becoming the dominant variant in England by late May.
The outcome of competition between variants depends on a wide range of factors such as intrinsic transmissibility, evasion of prior immunity, demographic specificities and interactions with non-pharmaceutical interventions. The presence and rise of non-B.1.1.7 variants in March likely was driven by importations and some community transmission. There was competition between non-B.1.17 variants which resulted in B.1.617.2 becoming dominant in April and May with considerable community transmission. Our results underscore that early detection of new variants requires a diverse array of data sources in community surveillance. Continued real-time information on the highly dynamic composition and trajectory of different SARS-CoV-2 lineages is essential to future control efforts.
National Institute for Health Research, Medicines and Healthcare products Regulatory Agency, DeepMind, EPSRC, EA Funds programme, Open Philanthropy, Academy of Medical Sciences Bill,Melinda Gates Foundation, Imperial College Healthcare NHS Trust, The Novo Nordisk Foundation, MRC Centre for Global Infectious Disease Analysis, Community Jameel, Cancer Research UK, Imperial College COVID-19 Research Fund, Medical Research Council, Wellcome Sanger Institute.
自2020年秋季出现以来,严重急性呼吸综合征冠状病毒2(SARS-CoV-2)的变异株B.1.1.7(世界卫生组织命名为阿尔法)迅速成为欧洲大部分地区的主要谱系。与此同时,全球还发现了其他几种变异株。与B.1.1.7不同,其中一些变异株具有被认为能导致部分免疫逃逸的突变。了解这些额外的变异株在B.1.1.7目前占主导地位的环境中何时以及如何构成威胁至关重要。
我们使用被动病例检测PCR数据、横断面社区感染调查、基因组监测和废水监测,研究了伦敦和英国其他地区非B.1.1.7谱系的流行趋势。研究期间为2021年1月31日至2021年5月15日。
从所有数据源来看,自2021年3月下旬以来,非B.1.1.7变异株的百分比一直在上升。这种上升最初是由多种具有免疫逃逸能力的谱系推动的。从4月中旬开始,B.1.617.2(世界卫生组织命名为德尔塔)迅速传播,到5月底成为英国的主要变异株。
变异株之间的竞争结果取决于多种因素,如内在传播性、对先前免疫的逃逸能力、人口统计学特征以及与非药物干预措施的相互作用。3月非B.1.1.7变异株的出现和增加可能是由输入病例和一些社区传播导致的。非B.1.17变异株之间存在竞争,导致B.1.617.2在4月和5月通过大量社区传播成为主要变异株。我们的结果强调,在社区监测中,早期发现新变异株需要多种数据源。持续获取关于不同SARS-CoV-2谱系高度动态组成和轨迹的实时信息对未来的防控工作至关重要。
英国国家卫生研究院、药品和医疗产品监管局、深度思考公司、工程和物理科学研究委员会、EA基金项目、开放慈善基金会、医学科学院比尔和梅琳达·盖茨基金会、帝国理工学院医疗保健国民保健服务信托基金、诺和诺德基金会、医学研究理事会全球传染病分析中心、社区贾米尔、英国癌症研究中心、帝国理工学院COVID-19研究基金、医学研究理事会、惠康桑格研究所。