Department of Radiology and Medical Imaging, University of Virginia, Charlottesville, VA.
F. Hoffmann-La Roche Ltd, Basel.
Haematologica. 2022 Jul 1;107(7):1633-1642. doi: 10.3324/haematol.2021.278663.
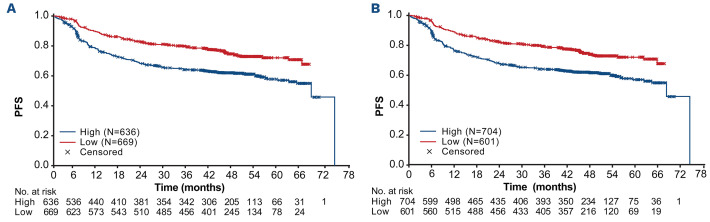
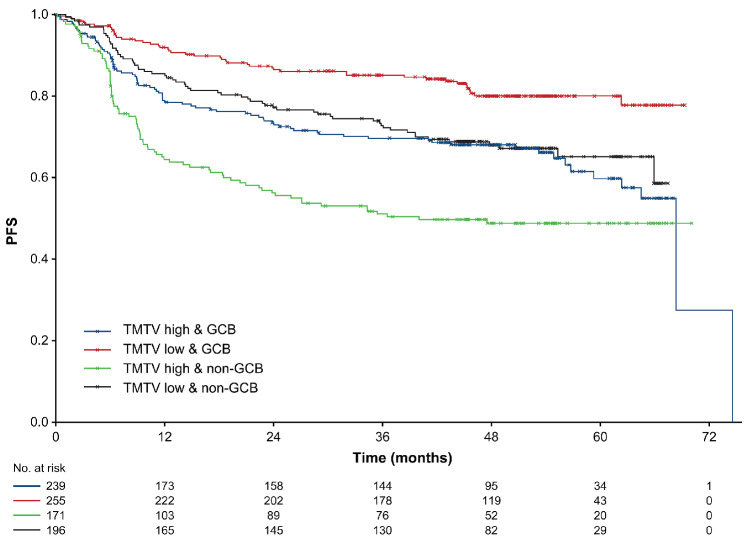
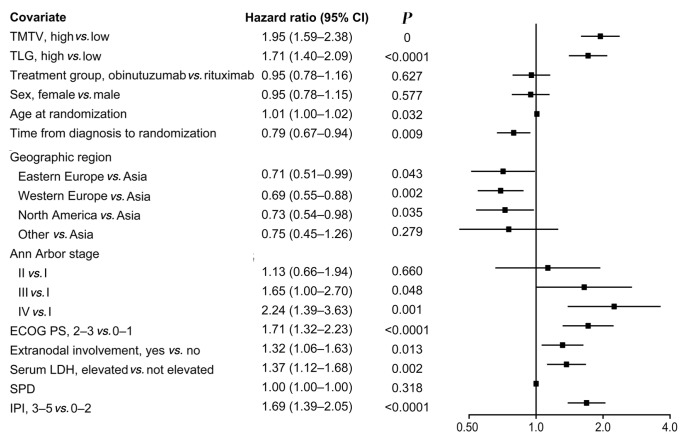
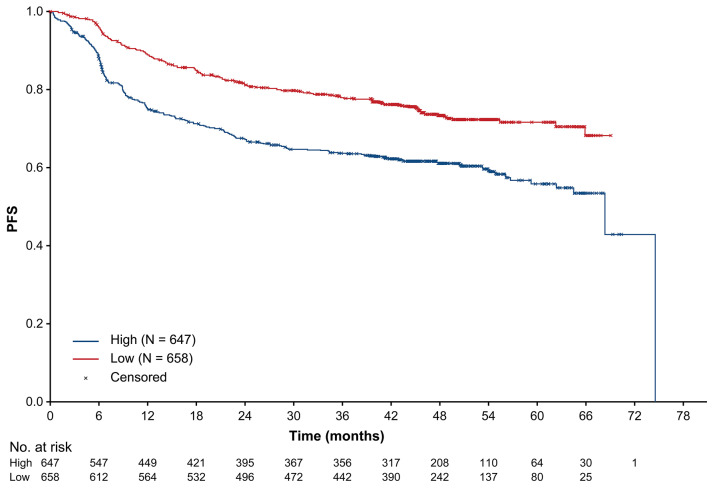
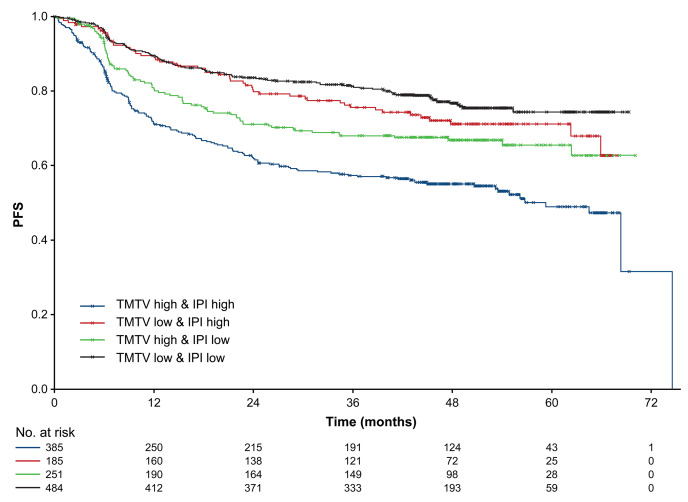
This retrospective analysis of the phase III GOYA study investigated the prognostic value of baseline metabolic tumor volume parameters and maximum standardized uptake values for overall and progression-free survival (PFS) in treatment-naïve diffuse large B-cell lymphoma. Baseline total metabolic tumor volume (determined for tumors >1 mL using a threshold of 1.5 times the mean liver standardized uptake value +2 standard deviations), total lesion glycolysis, and maximum standardized uptake value positron emission tomography data were dichotomized based on receiver operating characteristic analysis and divided into quartiles by baseline population distribution. Of 1,418 enrolled patients, 1,305 had a baseline positron emission tomography scan with detectable lesions. Optimal cut-offs were 366 cm3 for total metabolic tumor volume and 3,004 g for total lesion glycolysis. High total metabolic tumor volume and total lesion glycolysis predicted poorer PFS, with associations retained after adjustment for baseline and disease characteristics (high total metabolic tumor volume hazard ratio: 1.71, 95% confidence interval [CI]: 1.35- 2.18; total lesion glycolysis hazard ratio: 1.46; 95% CI: 1.15-1.86). Total metabolic tumor volume was prognostic for PFS in subgroups with International Prognostic Index scores 0-2 and 3-5, and those with different cell-of-origin subtypes. Maximum standardized uptake value had no prognostic value in this setting. High total metabolic tumor volume associated with high International Prognostic Index or non-germinal center B-cell classification identified the highest-risk cohort for unfavorable prognosis. In conclusion, baseline total metabolic tumor volume and total lesion glycolysis are independent predictors of PFS in patients with diffuse large B-cell lymphoma after first-line immunochemotherapy.
这项回顾性的 III 期 GOYA 研究分析了基线代谢肿瘤体积参数和最大标准化摄取值对初治弥漫性大 B 细胞淋巴瘤患者总生存和无进展生存(PFS)的预后价值。使用 1.5 倍肝脏标准化摄取值加 2 个标准差的阈值,对肿瘤体积大于 1ml 的肿瘤进行基线总代谢肿瘤体积(total metabolic tumor volume,TMTV)、总病变糖酵解和最大标准化摄取值正电子发射断层扫描(positron emission tomography,PET)数据的测定,根据接收者操作特征分析将其分为二分类,并根据基线人群分布分为四分位数。在 1418 名入组患者中,有 1305 名患者基线 PET 扫描有可检测病灶。最佳截断值为 TMTV 为 366cm3 和总病变糖酵解为 3004g。高 TMTV 和总病变糖酵解预测 PFS 较差,在调整基线和疾病特征后仍存在相关性(高 TMTV 危险比:1.71,95%置信区间[CI]:1.35-2.18;总病变糖酵解危险比:1.46;95%CI:1.15-1.86)。TMTV 在国际预后指数(International Prognostic Index,IPI)评分 0-2 和 3-5 以及不同细胞起源亚型的亚组中对 PFS 有预后价值。在这种情况下,最大标准化摄取值无预后价值。高 TMTV 与高 IPI 或非生发中心 B 细胞分类相关,确定了预后不良的最高风险亚组。总之,基线 TMTV 和总病变糖酵解是初治弥漫性大 B 细胞淋巴瘤患者一线免疫化疗后 PFS 的独立预测因子。