Nephrology, DIAMEDIKUM, Potsdam, Germany.
Apheresis Unit, Pentracor GmbH, Hennigsdorf, Germany.
Front Immunol. 2021 Aug 2;12:708101. doi: 10.3389/fimmu.2021.708101. eCollection 2021.
Plasma levels of C-reactive protein (CRP), induced by Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2) triggering COVID-19, can rise surprisingly high. The increase of the CRP concentration as well as a certain threshold concentration of CRP are indicative of clinical deterioration to artificial ventilation. In COVID-19, virus-induced lung injury and the subsequent massive onset of inflammation often drives pulmonary fibrosis. Fibrosis of the lung usually proceeds as sequela to a severe course of COVID-19 and its consequences only show months later. CRP-mediated complement- and macrophage activation is suspected to be the main driver of pulmonary fibrosis and subsequent organ failure in COVID-19. Recently, CRP apheresis was introduced to selectively remove CRP from human blood plasma.
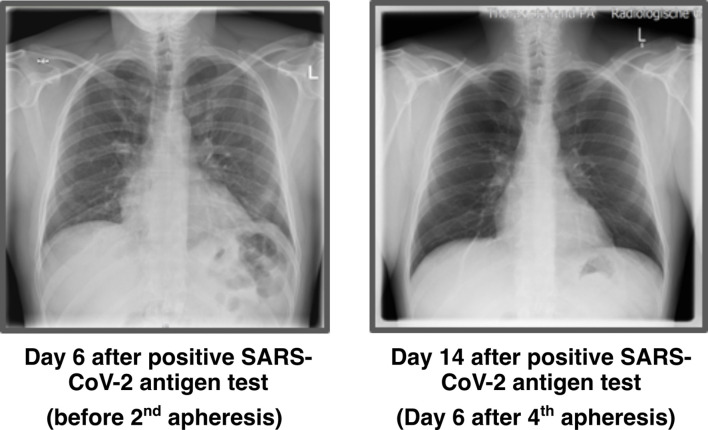
A 53-year-old, SARS-CoV-2 positive, male patient with the risk factor diabetes type 2 was referred with dyspnea, fever and fulminant increase of CRP. The patient's lungs already showed a pattern enhancement as an early sign of incipient pneumonia. The oxygen saturation of the blood was ≤ 89%. CRP apheresis using the selective CRP adsorber (PentraSorb CRP) was started immediately. CRP apheresis was performed peripheral venous access on 4 successive days. CRP concentrations before CRP apheresis ranged from 47 to 133 mg/l. The removal of CRP was very effective with up to 79% depletion within one apheresis session and 1.2 to 2.14 plasma volumes were processed in each session. No apheresis-associated side effects were observed. It was at no point necessary to transfer the patient to the Intensive Care Unit or to intubate him due to respiratory failure. 10 days after the first positive SARS-CoV-2 test, CRP levels stayed below 20 mg/l and the patient no longer exhibited fever. Fourteen days after the first positive SARS-CoV-2 test, the lungs showed no sign of pneumonia on X-ray.
This is the first report on CRP apheresis in an early COVID-19 patient with fulminant CRP increase. Despite a poor prognosis due to his diabetes and biomarker profile, the patient was not ventilated, and the onset of pneumonia was reverted.
严重急性呼吸综合征冠状病毒 2 (SARS-CoV-2)引发的 COVID-19 会导致 C 反应蛋白(CRP)的血浆水平出人意料地升高。CRP 浓度的增加以及 CRP 的某个阈值浓度表明需要进行人工通气以改善临床症状。在 COVID-19 中,病毒引起的肺损伤以及随后大量炎症的发生通常会导致肺纤维化。肺纤维化通常是 COVID-19 严重病程及其数月后后果的后遗症。CRP 介导的补体和巨噬细胞激活被怀疑是 COVID-19 中肺纤维化和随后器官衰竭的主要驱动因素。最近,CRP 血浆吸附法被引入以选择性地从人血浆中去除 CRP。
一名 53 岁男性 SARS-CoV-2 阳性患者,合并糖尿病 2 型这一危险因素,因呼吸困难、发热和 CRP 急剧升高而被转介。该患者的肺部已经出现了增强模式,这是肺炎早期的一个迹象。血液中的氧饱和度≤89%。立即开始使用选择性 CRP 吸附剂(PentraSorb CRP)进行 CRP 血浆吸附。在连续 4 天进行了外周静脉通路的 CRP 血浆吸附。在 CRP 血浆吸附前,CRP 浓度范围为 47-133mg/L。单次 CRP 血浆吸附的 CRP 去除率非常有效,可达 79%,每个疗程处理 1.2-2.14 个血浆容量。未观察到与 CRP 血浆吸附相关的副作用。患者从未因呼吸衰竭而需要转入重症监护病房或进行气管插管。首次 SARS-CoV-2 检测呈阳性后 10 天,CRP 水平保持在 20mg/L 以下,患者不再发热。首次 SARS-CoV-2 检测呈阳性后 14 天,X 光片显示肺部无肺炎迹象。
这是首例关于早期 COVID-19 患者 CRP 急剧升高时进行 CRP 血浆吸附的报告。尽管由于他的糖尿病和生物标志物特征导致预后不良,但患者未进行通气,肺炎发作得到逆转。