Saha Senjuti, Saha Sudipta, Kanon Naito, Hooda Yogesh, Islam Mohammad Shahidul, Islam Shuborno, Ahmed Zabed Bin, Rahman Sheikh Wasik, Alam Md Jahangir, Anik Ataul Mustufa, Sarkar Probir K, Ahsan Mohammed Rizwanul, Amin Md Ruhul, Saha Samir K
Child Health Research Foundation, Dhaka, Bangladesh.
Child Health Research Foundation, Dhaka, Bangladesh; Department of Social and Behavioral Sciences, Harvard T H Chan School of Public Health, Boston, MA, USA.
Lancet Glob Health. 2025 Jun;13(6):e1072-e1081. doi: 10.1016/S2214-109X(25)00048-8.
Respiratory syncytial virus (RSV) is a leading cause of paediatric hospital admissions worldwide, straining health systems. A lack of data on the burden of RSV infections and the impact on health systems in resource-limited settings hinders evidence-based policy decisions. Here, we aimed to assess RSV's burden on the health system in Bangladesh.
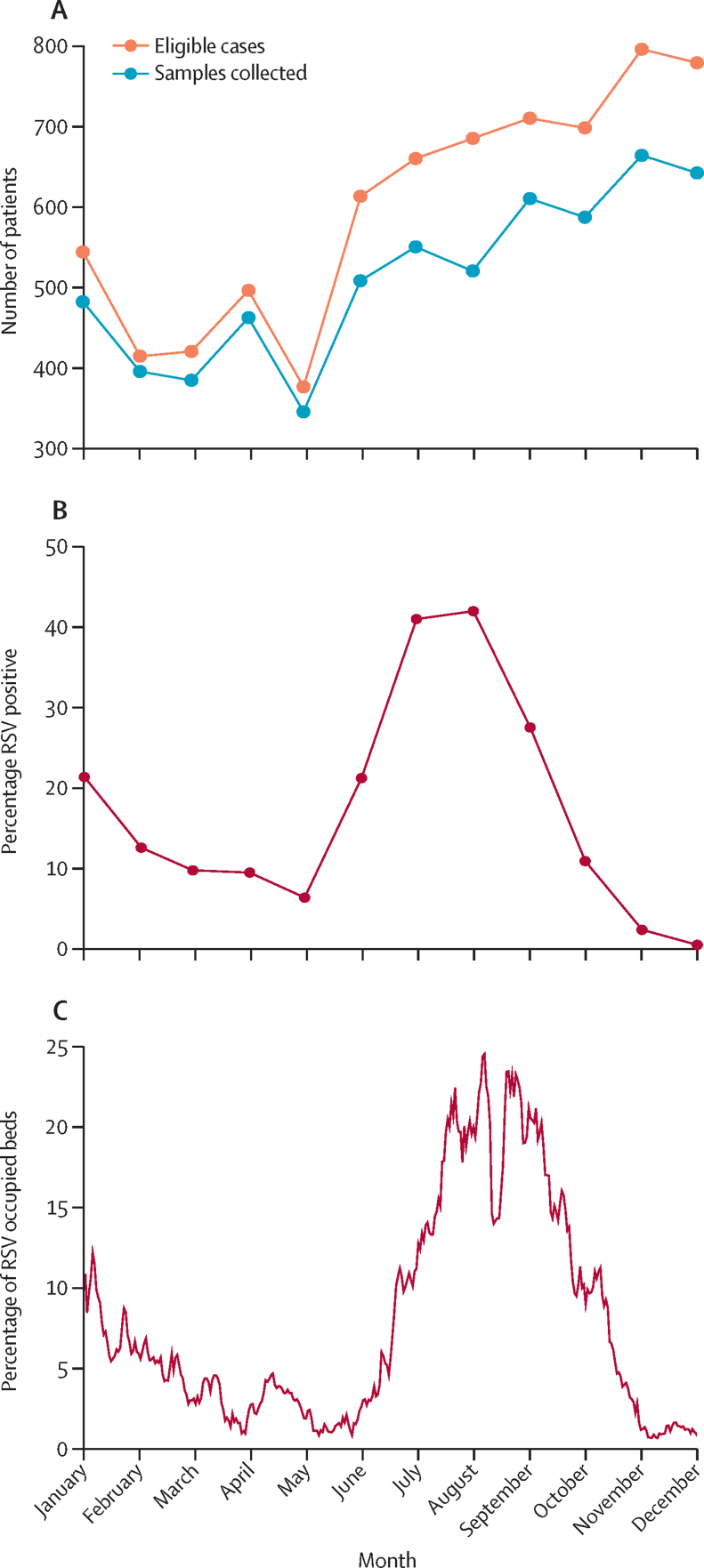
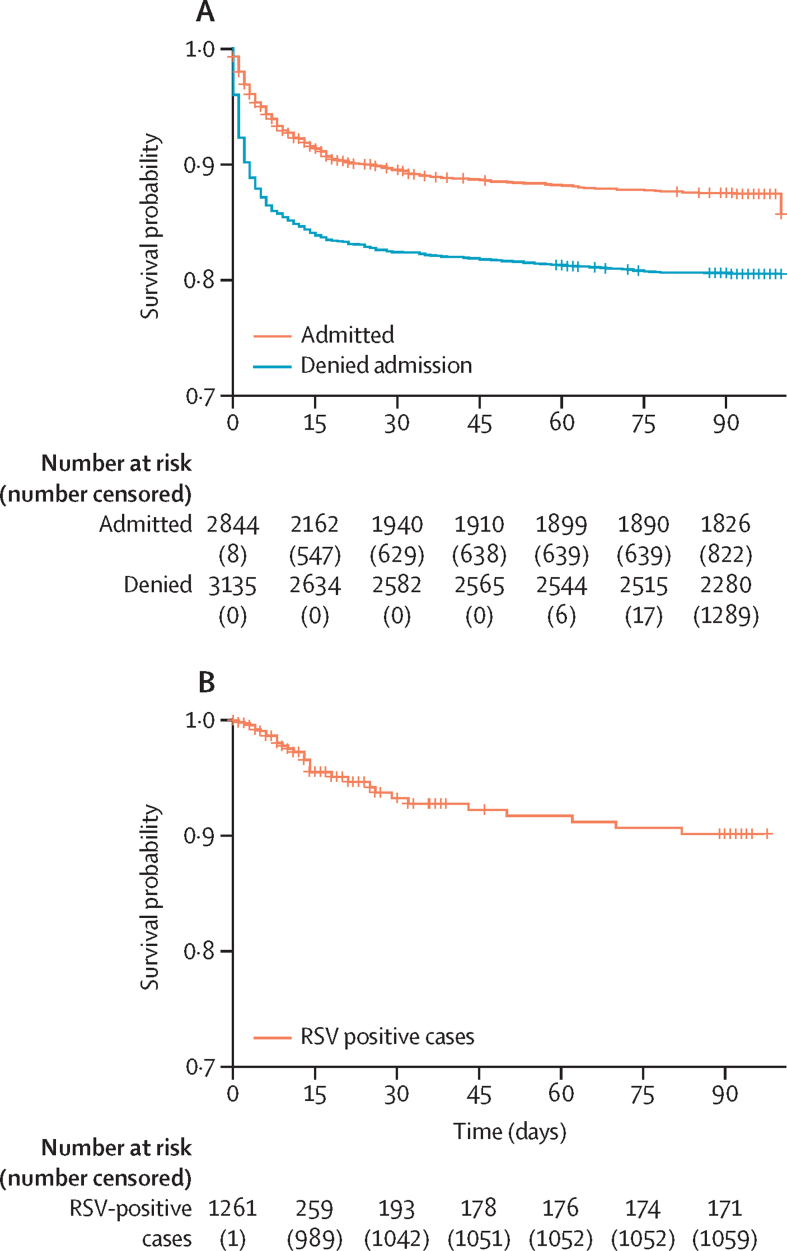
From January to December, 2019, we conducted a prospective study at Bangladesh's largest paediatric hospital among children aged 0-59 months admitted with a possible respiratory infection, as guided by the WHO RSV hospital-based surveillance case definition. Outcomes for RSV-positive children younger than 5 years were analysed. We also followed up outcomes of children denied hospitalisation due to bed shortages. Adjusted hazard ratios for children denied admission versus admitted were estimated using survival analysis. Monte Carlo simulations with a queueing model were used to estimate the effects of RSV prefusion F maternal vaccine or nirsevimab on admission denials and mortality.
Of 40 664 children admitted, 31 692 were younger than 5 years; 19 940 were in study wards. Among 7191 admitted with possible respiratory infections, 6149 (85·5%) had nasopharyngeal swabs taken, with 1261 (20·5%) testing RSV-positive. The median age of children who tested positive for RSV was 3·0 months (IQR 1·0-8·0), with a median hospital stay of 5 days (IQR 4-8); 24 (1·9%) of 1261 died in hospital. 8274 (5·5%) of 151 110 bed days were for children who were positive for RSV. Additionally, of 9169 children denied admission, outcomes were tracked for 3928 and compared with 2845 admitted. The hazard ratio for death was 1·56 (95% CI 1·34 to 1·81) for children denied versus admitted, being highest for neonates at 2·27 (1·87 to 2·75). RSV prefusion F maternal vaccine or nirsevimab could have reduced denials by 677 (95% prediction interval 63 to 1347) and 1289 (684 to 1865), respectively, potentially preventing 130 (-60 to 322) and 258 (32 to 469) deaths.
RSV strains health care in Bangladesh, increasing mortality risks. Preventive interventions could lessen its impact, boosting health-care capacity and child health in resource-limited settings.
The Bill & Melinda Gates Foundation.
呼吸道合胞病毒(RSV)是全球儿科住院的主要原因,给卫生系统带来了压力。资源有限地区缺乏关于RSV感染负担及其对卫生系统影响的数据,这阻碍了基于证据的政策决策。在此,我们旨在评估RSV在孟加拉国对卫生系统的负担。
2019年1月至12月,我们在孟加拉国最大的儿科医院对0至59个月因可能的呼吸道感染入院的儿童进行了一项前瞻性研究,该研究以世界卫生组织基于医院的RSV监测病例定义为指导。分析了5岁以下RSV阳性儿童的结局。我们还对因床位短缺而未住院儿童的结局进行了随访。使用生存分析估计未入院儿童与入院儿童的调整后风险比。使用排队模型进行蒙特卡洛模拟,以估计RSV预融合F母体疫苗或nirsevimab对入院拒绝和死亡率的影响。
在40664名入院儿童中,31692名年龄小于5岁;19940名在研究病房。在7191名因可能的呼吸道感染入院的儿童中,6149名(85.5%)采集了鼻咽拭子,其中1261名(20.5%)检测为RSV阳性。RSV检测呈阳性儿童的中位年龄为3.0个月(四分位间距1.0 - 8.0),中位住院时间为5天(四分位间距4 - 8);1261名中有24名(1.9%)在医院死亡。151110个床位日中有8274个(5.5%)是为RSV阳性儿童准备的。此外,在9169名未入院儿童中,对3928名儿童的结局进行了跟踪,并与2845名入院儿童进行了比较。未入院儿童与入院儿童的死亡风险比为1.56(95%置信区间1.34至1.81),新生儿最高,为2.27(1.87至2.75)。RSV预融合F母体疫苗或nirsevimab分别可减少677例(95%预测区间63至1347)和1289例(684至1865)入院拒绝,可能预防130例(-60至322)和258例(32至469)死亡。
RSV给孟加拉国医疗保健带来压力,增加了死亡风险。预防性干预措施可减轻其影响,增强资源有限地区的医疗保健能力并改善儿童健康状况。
比尔及梅琳达·盖茨基金会。