Peter Munk Cardiac Centre, Toronto General Hospital, University Health Network, University of Toronto, Toronto, Ontario, Canada.
Department of Cardiac Surgery, St Michael's Hospital, University of Toronto, Toronto, Ontario, Canada.
JAMA Netw Open. 2021 Aug 2;4(8):e2121867. doi: 10.1001/jamanetworkopen.2021.21867.
Postoperative atrial fibrillation (POAF) occurring after cardiac surgery is associated with adverse outcomes. Whether POAF persists beyond discharge is not well defined.
To determine whether continuous cardiac rhythm monitoring enhances detection of POAF among cardiac surgical patients during the first 30 days after hospital discharge compared with usual care.
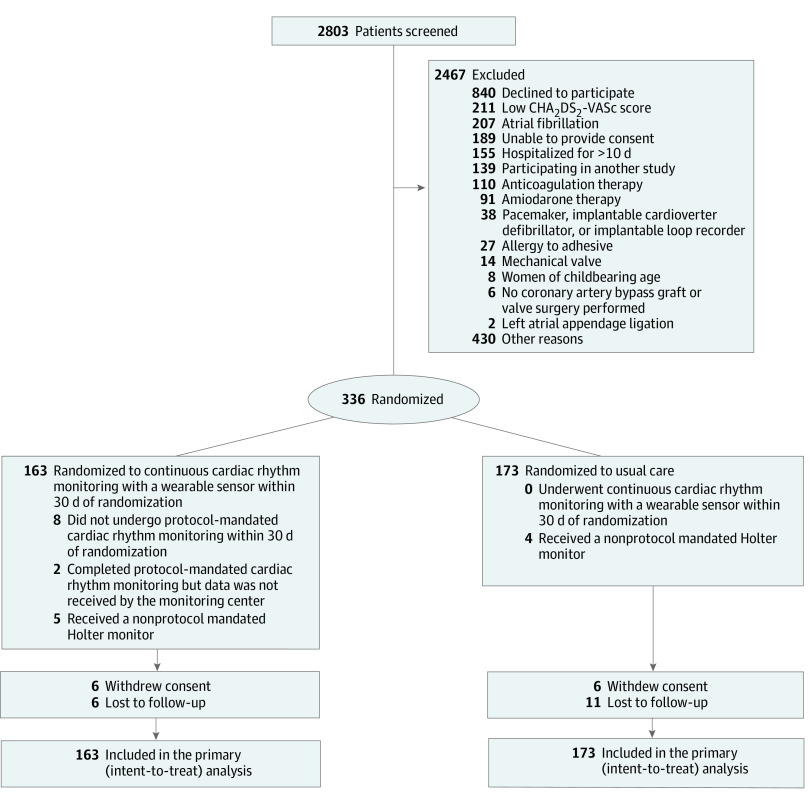
DESIGN, SETTING, AND PARTICIPANTS: This study is an investigator-initiated, open-label, multicenter, randomized clinical trial conducted at 10 Canadian centers. Enrollment spanned from March 2017 to March 2020, with follow-up through September 11, 2020. As a result of the COVID-19 pandemic, enrollment stopped on July 17, 2020, at which point 85% of the proposed sample size was enrolled. Cardiac surgical patients with CHA2DS2-VASc (congestive heart failure, hypertension, age ≥75 years, diabetes, prior stroke or transient ischemic attack, vascular disease, age 65-74 years, female sex) score greater than or equal to 4 or greater than or equal to 2 with risk factors for POAF, no history of preoperative AF, and POAF lasting less than 24 hours during hospitalization were enrolled.
The intervention group underwent continuous cardiac rhythm monitoring with wearable, patch-based monitors for 30 days after randomization. Monitoring was not mandated in the usual care group within 30 days after randomization.
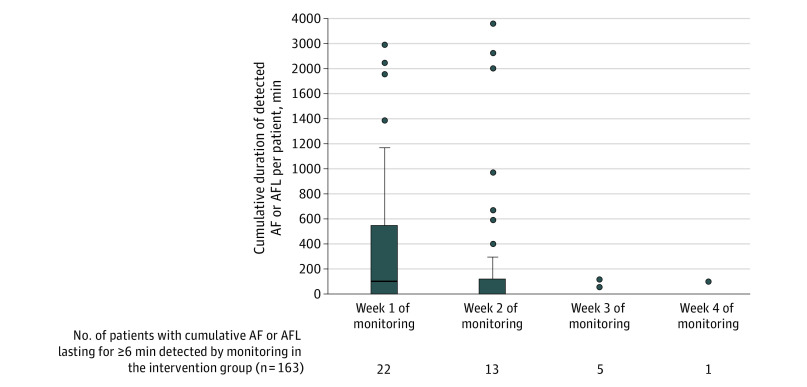
The primary outcome was cumulative AF and/or atrial flutter lasting 6 minutes or longer detected by continuous cardiac rhythm monitoring or by a 12-lead electrocardiogram within 30 days of randomization. Prespecified secondary outcomes included cumulative AF lasting 6 hours or longer and 24 hours or longer within 30 days of randomization, death, myocardial infarction, ischemic stroke, non-central nervous system thromboembolism, major bleeding, and oral anticoagulation prescription.
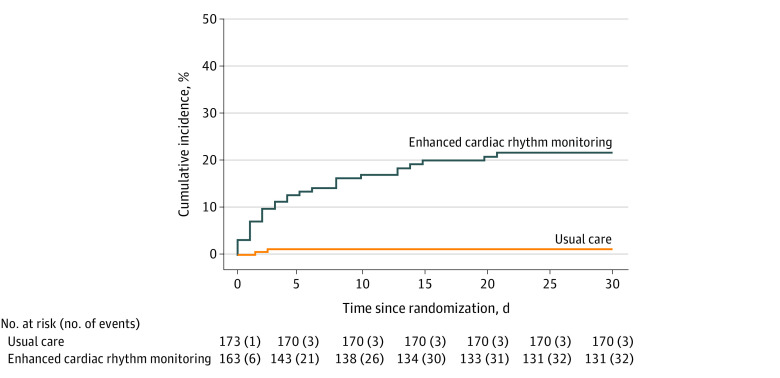
Of the 336 patients randomized (163 patients in the intervention group and 173 patients in the usual care group; mean [SD] age, 67.4 [8.1] years; 73 women [21.7%]; median [interquartile range] CHA2DS2-VASc score, 4.0 [3.0-4.0] points), 307 (91.4%) completed the trial. In the intent-to-treat analysis, the primary end point occurred in 32 patients (19.6%) in the intervention group vs 3 patients (1.7%) in the usual care group (absolute difference, 17.9%; 95% CI, 11.5%-24.3%; P < .001). AF lasting 6 hours or longer was detected in 14 patients (8.6%) in the intervention group vs 0 patients in the usual care group (absolute difference, 8.6%; 95% CI, 4.3%-12.9%; P < .001).
In post-cardiac surgical patients at high risk of stroke, no preoperative AF history, and AF lasting less than 24 hours during hospitalization, continuous monitoring revealed a significant increase in the rate of POAF after discharge that would otherwise not be detected by usual care. Studies are needed to examine whether these patients will benefit from oral anticoagulation therapy.
ClinicalTrials.gov Identifier: NCT02793895.
心脏手术后发生的房性心动过速(POAF)与不良结局相关。POAF 是否在出院后持续存在尚不清楚。
确定与常规护理相比,在出院后 30 天内,连续心脏节律监测是否能提高心脏手术后患者 POAF 的检出率。
设计、地点和参与者:这是一项由研究者发起的、开放性、多中心、随机临床试验,在加拿大的 10 个中心进行。招募工作从 2017 年 3 月持续到 2020 年 3 月,随访至 2020 年 9 月 11 日。由于 COVID-19 大流行,招募工作于 2020 年 7 月 17 日停止,此时已经招募了计划样本量的 85%。CHA2DS2-VASc(充血性心力衰竭、高血压、年龄≥75 岁、糖尿病、既往卒中或短暂性脑缺血发作、血管疾病、年龄 65-74 岁、女性)评分大于等于 4 分或大于等于 2 分且有 POAF 风险因素、无术前 AF 病史和住院期间 POAF 持续时间小于 24 小时的心脏手术患者被纳入研究。
干预组在随机分组后 30 天内接受连续心脏节律监测,使用可穿戴、贴片式监测器。在随机分组后 30 天内,常规护理组不强制进行监测。
主要结局是在随机分组后 30 天内通过连续心脏节律监测或 12 导联心电图检测到的持续 6 分钟或更长时间的 AF 和/或心房扑动。预设的次要结局包括随机分组后 30 天内持续 6 小时或更长时间和 24 小时或更长时间的 AF、死亡、心肌梗死、缺血性卒中和非中枢神经系统血栓栓塞、大出血和口服抗凝药物处方。
在随机分组的 336 例患者中(干预组 163 例,常规护理组 173 例;平均[标准差]年龄 67.4[8.1]岁;73 名女性[21.7%];中位数[四分位间距]CHA2DS2-VASc 评分 4.0[3.0-4.0]分),307 例(91.4%)完成了试验。在意向治疗分析中,主要终点在干预组的 32 例患者(19.6%)和常规护理组的 3 例患者(1.7%)中发生(绝对差异,17.9%;95%置信区间,11.5%-24.3%;P<0.001)。在干预组的 14 例患者(8.6%)中检测到持续 6 小时或更长时间的 AF,而常规护理组的 0 例患者中未检测到(绝对差异,8.6%;95%置信区间,4.3%-12.9%;P<0.001)。
在心脏手术后有中风高风险、无术前 AF 病史和住院期间 AF 持续时间小于 24 小时的患者中,连续监测显示 POAF 的发生率显著增加,而常规护理则无法检测到。需要研究这些患者是否会受益于口服抗凝治疗。
ClinicalTrials.gov 标识符:NCT02793895。