Blitz Sarah E, Bernstock Joshua D, Dmytriw Adam A, Ditoro Daniel Francis, Kappel Ari D, Gormley William B, Peruzzi Pierpaolo
Harvard Medical School, Boston, MA, United States.
Department of Neurosurgery, Brigham and Women's Hospital, Harvard University, Boston, MA, United States.
Front Surg. 2021 Aug 11;8:714771. doi: 10.3389/fsurg.2021.714771. eCollection 2021.
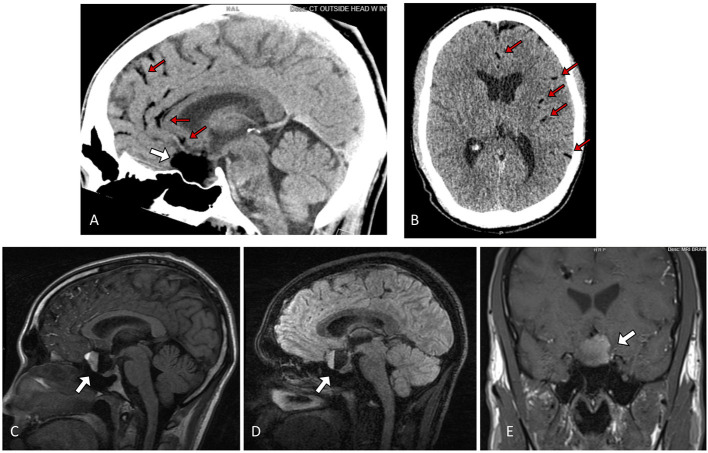
Ruptured intracranial dermoid cysts are extremely rare. Standard treatment consists of endonasal decompression or craniotomy with evacuation and copious irrigation of subarachnoid spaces to remove any disseminated cystic contents. Disseminated fat particles in the subarachnoid space may be the cause of further sequalae, including the subsequent development of chemical meningitis and hydrocephalus. Here, we present a case of ruptured suprasellar dermoid cyst treated with craniotomy for emergent optic nerve decompression, followed by postoperative hydrocephalus successfully treated with lumbar drain. We describe a 30-year-old man with a history of migraines who presented with acute onset of headache, photophobia, nausea, vomiting, and vision loss in the left eye. Head CT and brain MRI demonstrated a ruptured suprasellar dermoid cyst with associated mass effect on the optic nerves and frontal lobes as well as fat attenuation material within the subarachnoid spaces. The patient underwent left frontotemporal craniotomy for cyst resection and developed non-obstructive hydrocephalus on postoperative day 1, refractory to external ventricular drainage. Placement of a lumbar drain cleared the subarachnoid space of debris derived from the ruptured dermoid cyst, and the hydrocephalus resolved. The patient did not require permanent CSF diversion. Intracranial dermoid cysts are uncommon, and rupture is a rare event. Standard surgical treatment with craniotomy for evacuation may leave disseminated dermoid contents and fat particles throughout the subarachnoid spaces. We highlight a case of ruptured suprasellar dermoid cyst with postoperative communicating hydrocephalus treated with lumbar drain when external ventricular drain (EVD) was ineffective. Review of the current literature reveals inconsistent findings on the effects of remaining fat particles. In cases with clinical evidence of increased intracranial pressure due to non-obstructive hydrocephalus attributable to chemical meningitis, temporary lumbar drainage is an option to be considered before committing the patient to permanent shunting.
颅内皮样囊肿破裂极为罕见。标准治疗方法包括经鼻减压或开颅手术,清除囊肿并大量冲洗蛛网膜下腔以清除任何播散的囊肿内容物。蛛网膜下腔内播散的脂肪颗粒可能是导致进一步后遗症的原因,包括随后发生的化学性脑膜炎和脑积水。在此,我们报告一例鞍上破裂皮样囊肿患者,该患者接受开颅手术以紧急减压视神经,术后发生脑积水,随后通过腰大池引流成功治疗。我们描述了一名30岁有偏头痛病史的男性,其出现急性头痛、畏光、恶心、呕吐及左眼视力丧失。头颅CT和脑部MRI显示鞍上破裂皮样囊肿,对视神经和额叶有相关占位效应,蛛网膜下腔内有脂肪密度物质。患者接受左额颞开颅囊肿切除术,术后第1天出现非梗阻性脑积水,脑室引流无效。放置腰大池引流清除了破裂皮样囊肿产生的蛛网膜下腔碎屑,脑积水得以缓解。患者无需永久性脑脊液分流。颅内皮样囊肿并不常见,破裂更是罕见事件。采用开颅手术清除囊肿的标准外科治疗可能会在蛛网膜下腔内留下播散的皮样囊肿内容物和脂肪颗粒。我们强调了一例鞍上破裂皮样囊肿术后交通性脑积水患者,在脑室引流无效时采用腰大池引流治疗的病例。回顾当前文献发现,关于残留脂肪颗粒的影响存在不一致的结果。对于因化学性脑膜炎导致非梗阻性脑积水而有颅内压升高临床证据的病例,在决定患者进行永久性分流之前,临时腰大池引流是一种可考虑的选择。