Department of Pharmacy and Pharmacology, University of Bath, Bath, BA2 7AY, UK.
Pharmacy Research Centre, University Hospital Southampton, Southampton, SO16 6YD, UK.
BMC Med. 2021 Aug 31;19(1):189. doi: 10.1186/s12916-021-02067-5.
Anticoagulation for stroke prevention in atrial fibrillation (AF) has, historically, been under-used in older people. The aim of this study was to investigate prescribing of oral anticoagulants (OACs) for people aged ≥ 75 years in the UK before and after direct oral anticoagulants (DOACs) became available.
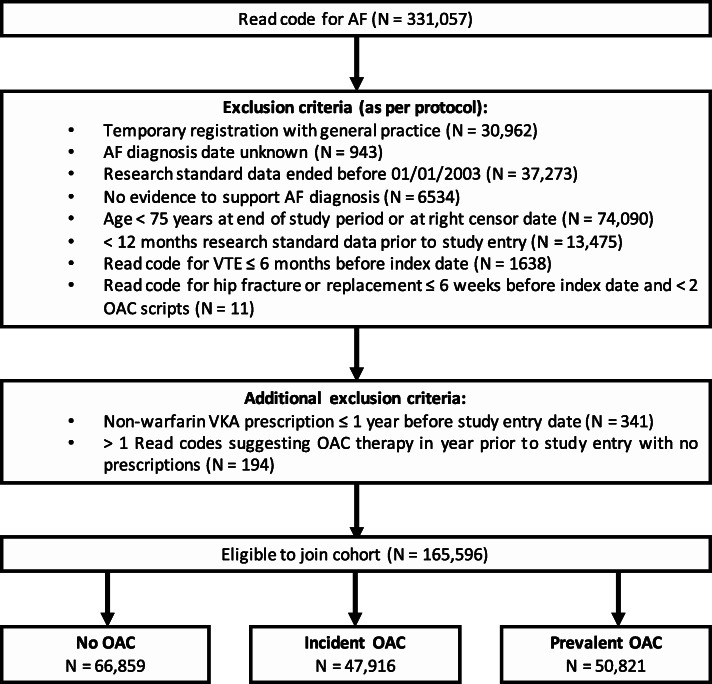
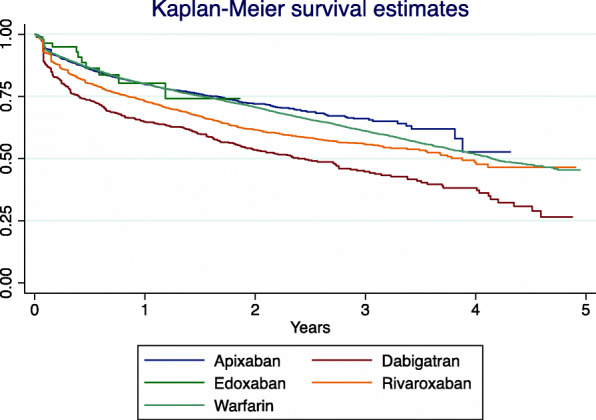
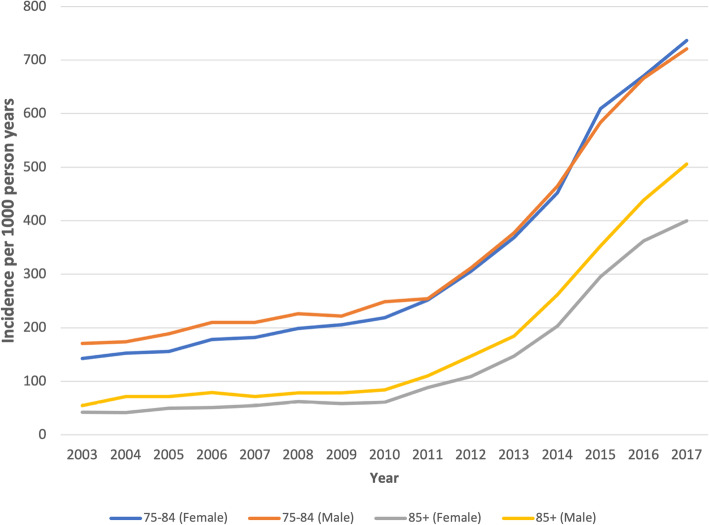
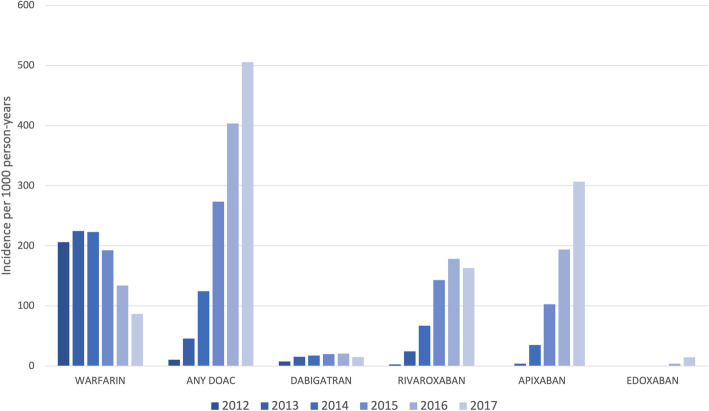
A cohort of patients aged ≥ 75 years with a diagnosis of AF was derived from the Clinical Practice Research Datalink (CPRD) between January 1, 2003, and December 27, 2017. Patients were grouped as no OAC, incident OAC (OAC newly prescribed) or prevalent OAC (entered study on OAC). Incidence and point prevalence of OAC prescribing were calculated yearly. The risk of being prescribed an OAC if a co-morbidity was present was calculated; the risk difference (RD) was reported. Kaplan-Meier curves were used to explore persistence with anticoagulation. A Cox regression was used to model persistence with warfarin and DOACs over time.
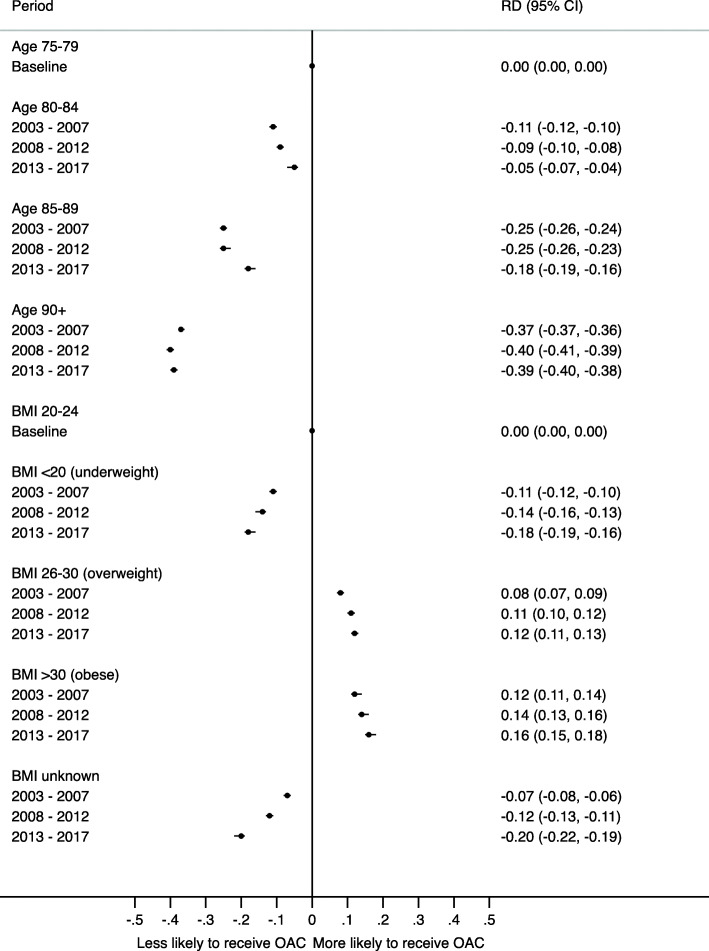
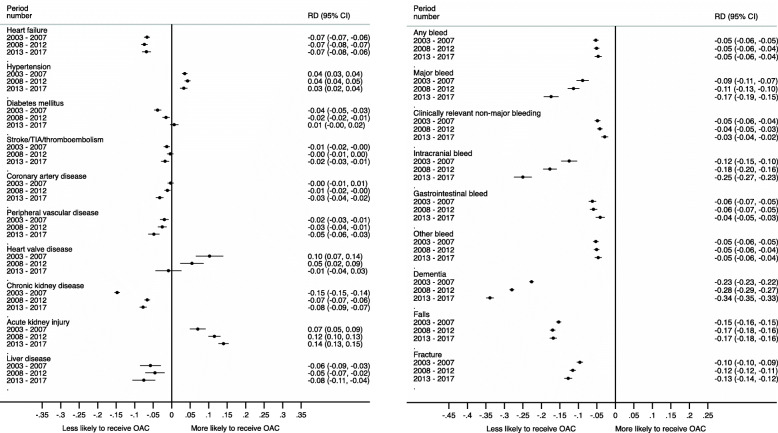
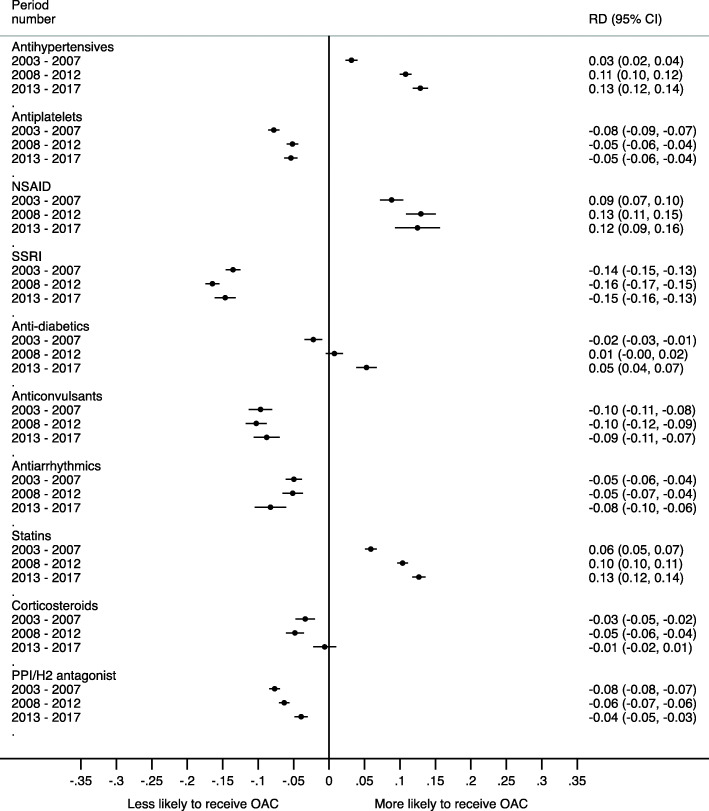
The cohort comprised 165,596 patients (66,859 no OAC; 47,916 incident OAC; 50,821 prevalent OAC). Incidence of OAC prescribing increased from 111 per 1000 person-years in 2003 to 587 per 1000 person-years in 2017. Older patients (≥ 90 years) were 40% less likely to receive an OAC (RD -0.40, 95% CI -0.41 to -0.39) than younger individuals (75-84 years). The likelihood of being prescribed an OAC was lower with a history of dementia (RD -0.34, 95% CI -0.35 to -0.33), falls (RD -0.17, 95% CI -0.18 to -0.16), major bleeds (RD -0.17, 95% CI -0.19 to -0.15) and fractures (RD -0.13, 95% CI -0.14 to -0.12). Persistence with warfarin was higher than DOACs in the first year (0-1 year: HR 1.25, 95% CI 1.17-1.33), but this trend reversed by the third year of therapy (HR 0.75, 95% CI 0.63-0.89).
OAC prescribing for older people with AF has increased; however, substantial disparities persist with age and co-morbidities. Whilst OACs should not be withheld solely due to the risk of falls, these results do not reflect this national guidance. Furthermore, the under-prescribing of OACs for patients with dementia or advancing age may be due to decisions around risk-benefit management.
EUPAS29923 . First registered on: 27/06/2019.
在房颤(AF)患者中,历史上抗凝治疗在老年人中应用不足。本研究旨在调查在直接口服抗凝剂(DOAC)问世前后,英国≥75 岁人群中口服抗凝剂(OAC)的使用情况。
从 2003 年 1 月 1 日至 2017 年 12 月 27 日,从临床实践研究数据链(CPRD)中提取了一组≥75 岁的房颤患者。将患者分为无 OAC、新发 OAC(新处方 OAC)或已有 OAC(入组时正在使用 OAC)。每年计算 OAC 处方的发生率和时点患病率。计算有合并症时使用 OAC 的风险,并报告风险差异(RD)。使用 Kaplan-Meier 曲线探讨抗凝治疗的持久性。使用 Cox 回归模型随时间推移分析华法林和 DOAC 治疗的持久性。
该队列包括 165596 名患者(66859 名无 OAC;47916 名新发 OAC;50821 名已有 OAC)。OAC 处方的发生率从 2003 年的每 1000 人年 111 例增加到 2017 年的每 1000 人年 587 例。≥90 岁的老年患者(RD-0.40,95%CI-0.41 至-0.39)接受 OAC 的可能性比 75-84 岁的年轻患者低 40%。有痴呆史(RD-0.34,95%CI-0.35 至-0.33)、跌倒史(RD-0.17,95%CI-0.18 至-0.16)、大出血史(RD-0.17,95%CI-0.19 至-0.15)和骨折史(RD-0.13,95%CI-0.14 至-0.12)的患者使用 OAC 的可能性较低。第一年(0-1 年)华法林的持久性高于 DOACs(HR1.25,95%CI1.17-1.33),但在治疗的第三年,这种趋势发生逆转(HR0.75,95%CI0.63-0.89)。
≥75 岁的房颤患者中 OAC 的使用有所增加;然而,年龄和合并症仍然存在显著差异。尽管不应仅仅因为跌倒风险而拒绝使用 OAC,但这些结果并没有反映这一国家指南。此外,痴呆或高龄患者 OAC 使用率低可能是由于风险效益管理方面的决策。
EUPAS29923。首次注册日期:2019 年 6 月 27 日。