Department of Surgical Pathology, Sapporo Medical University, School of Medicine, South 1, West 16, Chuo-ku, Sapporo, Hokkaido, 060-8543, Japan.
Department of Orthopedic Surgery, Sapporo Medical University, School of Medicine, Sapporo, Hokkaido, 060-8543, Japan.
Diagn Pathol. 2021 Aug 30;16(1):79. doi: 10.1186/s13000-021-01140-0.
A definitive diagnosis of malignant peripheral nerve sheath tumor (MPNST) is challenging, especially in cases without neurofibromatosis 1 (NF1), because MPNST lacks specific markers on immunohistochemistry (IHC).
We performed IHC for histone 3 trimethylated on lysine 27 (H3K27me3) and evaluated the percentage of cells with H3K27me3 loss using measured values at 10% intervals, categorized as complete loss (100% of tumor cells lost staining), partial loss (10% to 90% of tumor cells lost staining), and intact (no tumor cells lost staining). We conducted fluorescence in situ hybridization (FISH) for NF1 and p16 deletions comparing 55 MPNSTs and 35 non-MPNSTs, consisting of 9 synovial sarcomas (SSs), 8 leiomyosarcomas (LMSs), 10 myxofibrosarcomas (MFSs), and 8 undifferentiated pleomorphic sarcomas (UPSs). We assessed the percentage of cells with homozygous and heterozygous deletions and defined "deletion" if the percentage of either the NF1 or p16 deletion signals was greater than 50% of tumor cells.
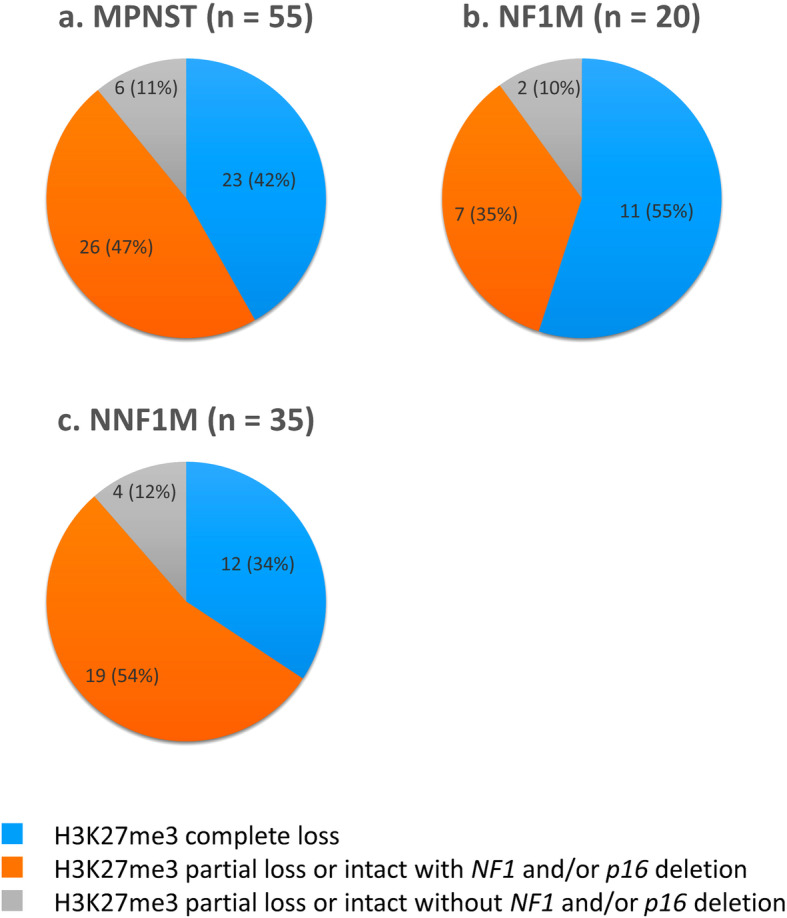
Among the 55 MPNSTs, 23 (42%) showed complete H3K27me3 loss and 32 (58%) exhibited partial loss or intact. One each of the 9 SSs (11%), 8 LMSs (12%), and 8 UPSs (12%) showed complete H3K27me3 loss and many non-MPNSTs exhibited intact or partial H3K27me3 loss. Among the 55 MPNSTs, 33 (60%) and 44 (80%) showed NF1 or p16 deletion, respectively. Co-deletion of NF1 and p16 was observed in 29 (53%) MPNSTs. Among the 23 MPNTSs showing H3K27me3 complete loss, 18 (78%) and 20 (87%) exhibited NF1 or p16 deletion, respectively. Among the 32 MPNSTs with H3K27me3 partial loss or intact, 15 (47%) and 24 (75%) exhibited NF1 or p16 deletion, respectively. The frequency of NF1 and/or p16 deletion tended to be lower in non-MPNSTs than in MPNSTs. Approximately 90% of MPNSTs included cases with H3K27me3 complete loss and cases showing H3K27me3 partial loss or intact with NF1 and/or p16 deletion. Approximately 50% of MPNSTs showed co-deletion of NF1 and p16 regardless of H3K27me3 loss.
FISH for NF1 and p16 deletions, frequently observed in high-grade MPNSTs, might be a useful ancillary diagnostic tool for differentiating MPNST from other mimicking spindle cell and pleomorphic sarcomas.
在没有神经纤维瘤病 1 型(NF1)的情况下,恶性外周神经鞘瘤(MPNST)的明确诊断具有挑战性,因为 MPNST 在免疫组织化学(IHC)上缺乏特异性标志物。
我们对组蛋白 3 赖氨酸 27 三甲基化(H3K27me3)进行 IHC,并使用 10%间隔的测量值评估 H3K27me3 缺失的细胞百分比,分为完全缺失(100%的肿瘤细胞失去染色)、部分缺失(10%至 90%的肿瘤细胞失去染色)和完整(无肿瘤细胞失去染色)。我们对 NF1 和 p16 缺失进行了荧光原位杂交(FISH)比较了 55 例 MPNST 和 35 例非 MPNST,包括 9 例滑膜肉瘤(SSs)、8 例平滑肌肉瘤(LMSs)、10 例黏液纤维肉瘤(MFSs)和 8 例未分化多形性肉瘤(UPSs)。我们评估了具有纯合和杂合缺失的细胞百分比,并将 NF1 或 p16 缺失信号的百分比大于肿瘤细胞的 50%定义为“缺失”。
在 55 例 MPNST 中,23 例(42%)表现出完全的 H3K27me3 缺失,32 例(58%)表现出部分缺失或完整。9 例 SSs(11%)、8 例 LMSs(12%)和 8 例 UPSs(12%)各有 1 例表现出完全的 H3K27me3 缺失,许多非 MPNST 表现出完整或部分 H3K27me3 缺失。在 55 例 MPNST 中,分别有 33 例(60%)和 44 例(80%)显示 NF1 或 p16 缺失。在 29 例(53%)表现出 H3K27me3 完全缺失的 MPNST 中,分别有 18 例(78%)和 20 例(87%)显示 NF1 或 p16 缺失。在 32 例 H3K27me3 部分缺失或完整的 MPNST 中,分别有 15 例(47%)和 24 例(75%)显示 NF1 或 p16 缺失。NF1 和/或 p16 缺失的频率在非 MPNST 中似乎低于 MPNST。大约 90%的 MPNST 包括 H3K27me3 完全缺失的病例和 H3K27me3 部分缺失或完整且 NF1 和/或 p16 缺失的病例。大约 50%的 MPNST 显示 NF1 和 p16 的共缺失,无论 H3K27me3 是否缺失。
在高级别 MPNST 中经常观察到 NF1 和 p16 缺失的 FISH 可能是区分 MPNST 与其他模仿梭形细胞和多形性肉瘤的有用辅助诊断工具。