Medical University of South Carolina, 135 Rutledge Ave, MSC 561, Charleston, SC, 29425, USA.
The Children's Hospital at Montefiore, 111 East 210th Street, Bronx, NY, 10467, USA.
Pediatr Rheumatol Online J. 2021 Aug 30;19(1):137. doi: 10.1186/s12969-021-00627-w.
Consensus treatment plans have been developed for induction therapy of newly diagnosed proliferative lupus nephritis (LN) in childhood-onset systemic lupus erythematosus. However, patients who do not respond to initial therapy, or who develop renal flare after remission, warrant escalation of treatment. Our objective was to assess current practices of pediatric nephrologists and rheumatologists in North America in treatment of refractory proliferative LN and flare.
Members of Childhood Arthritis and Rheumatology Research Alliance (CARRA) and the American Society for Pediatric Nephrology (ASPN) were surveyed in November 2015 to assess therapy choices (other than modifying steroid dosing) and level of agreement between rheumatologists and nephrologists for proliferative LN patients. Two cases were presented: (1) refractory disease after induction treatment with corticosteroid and cyclophosphamide (CYC) and (2) nephritis flare after initial response to treatment. Survey respondents chose treatments for three follow up scenarios for each case that varied by severity of presentation. Treatment options included CYC, mycophenolate mofetil (MMF), rituximab (RTX), and others, alone or in combination.
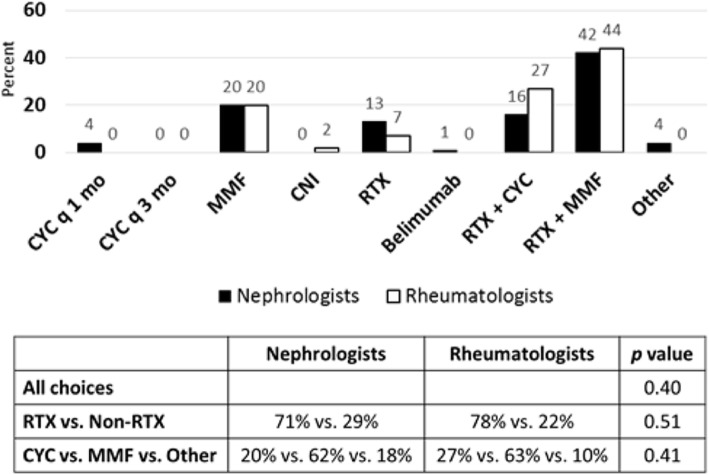
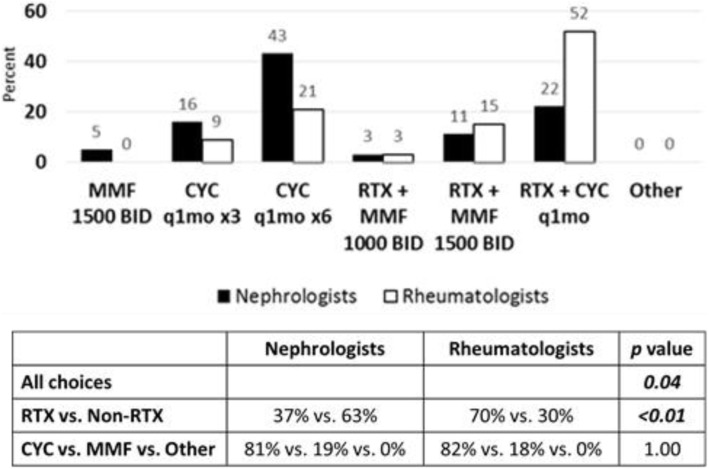
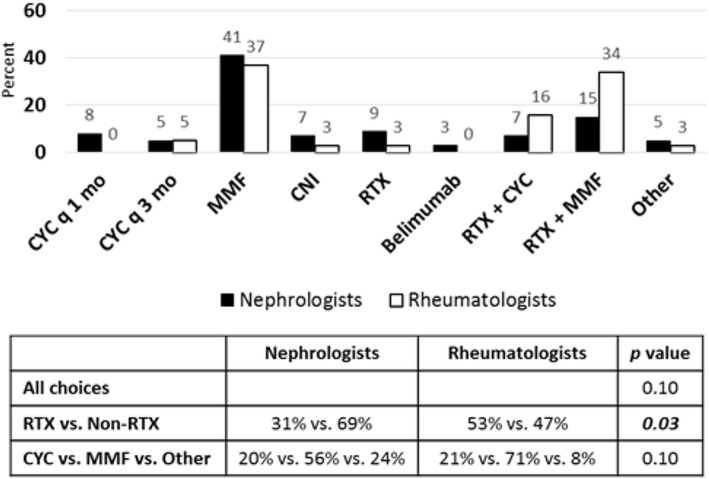
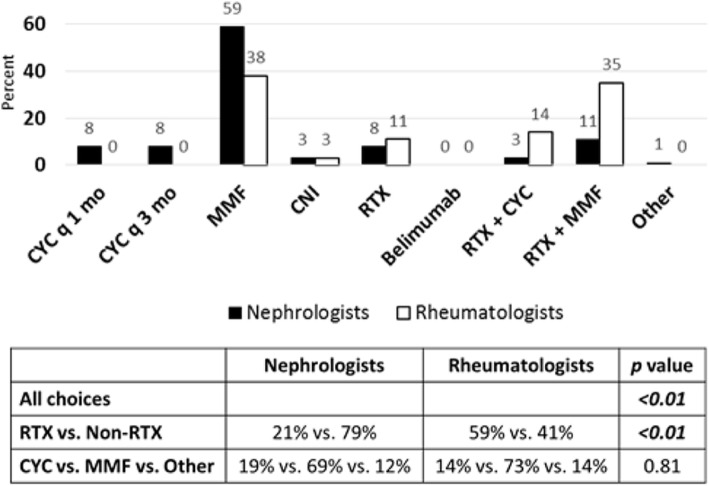
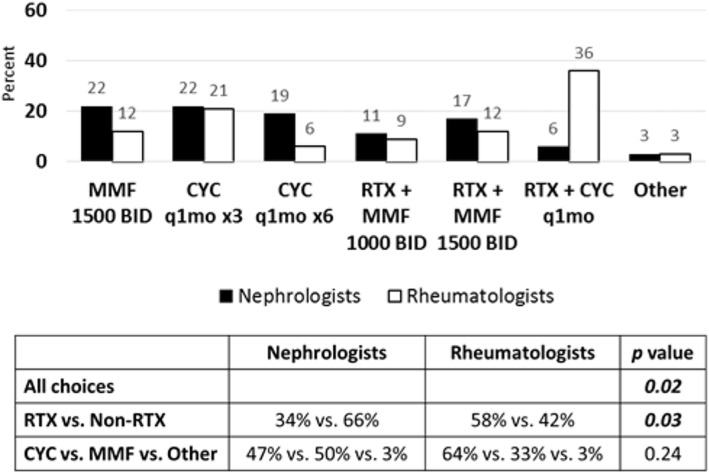
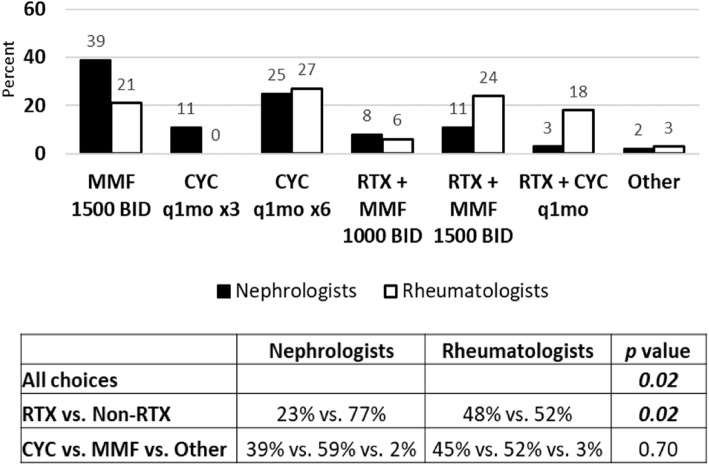
Seventy-six respondents from ASPN and foty-one respondents from CARRA represented approximately 15 % of the eligible members from each organization. Treatment choices between nephrologists and rheumatologists were highly variable and received greater than 50 % agreement for an individual treatment choice in only the following 2 of 6 follow up scenarios: 59 % of nephrologists, but only 38 % of rheumatologists, chose increasing dose of MMF in the case of LN refractory to induction therapy with proteinuria, hematuria, and improved serum creatinine. In a follow up scenario showing severe renal flare after achieving remission with induction therapy, 58 % of rheumatologists chose CYC and RTX combination therapy, whereas the top choice for nephrologists (43 %) was CYC alone. Rheumatologists in comparison to nephrologists chose more therapy options that contained RTX in all follow up scenarios except one (p < 0.05).
Therapy choices for pediatric rheumatologists and nephrologists in the treatment of refractory LN or LN flare were highly variable with rheumatologists more often choosing rituximab. Further investigation is necessary to delineate the reasons behind this finding. This study highlights the importance of collaborative efforts in developing consensus treatment plans for pediatric LN.
已为儿童发病的系统性红斑狼疮(SLE)新诊断的增生性狼疮肾炎(LN)诱导治疗制定了共识治疗方案。但是,对于初始治疗无反应或缓解后出现肾复发的患者,需要升级治疗。我们的目的是评估北美儿科肾脏病学家和风湿病学家在治疗难治性增生性 LN 和复发方面的当前实践。
2015 年 11 月,对儿童关节炎和风湿病研究联盟(CARRA)和美国儿科学会肾脏病学会(ASPN)的成员进行了调查,以评估治疗选择(除了调整类固醇剂量之外)以及风湿病学家和肾脏病学家对增生性 LN 患者的治疗选择的一致性。提出了两种情况:(1)用皮质类固醇和环磷酰胺(CYC)进行诱导治疗后的难治性疾病;(2)初始治疗后出现肾炎复发。根据表现严重程度的不同,每位患者的每种情况都有三种后续治疗方案,调查对象选择了不同的治疗方案。治疗选择包括 CYC、霉酚酸酯(MMF)、利妥昔单抗(RTX)和其他药物,单独或联合使用。
ASPN 有 76 名受访者,CARRA 有 41 名受访者,分别代表了各自组织中大约 15%的合格成员。肾脏病学家和风湿病学家的治疗选择差异很大,只有在以下 6 种后续治疗方案中的 2 种方案中,对于单一治疗选择的意见一致性超过 50%:59%的肾脏病学家,但只有 38%的风湿病学家,选择在 LN 对诱导治疗无反应且蛋白尿、血尿和血清肌酐改善的情况下增加 MMF 的剂量。在诱导治疗缓解后出现严重肾复发的情况下,58%的风湿病学家选择 CYC 和 RTX 联合治疗,而肾脏病学家的首选(43%)是 CYC 单药。与肾脏病学家相比,在所有后续治疗方案中,除了一种方案外(p<0.05),风湿病学家选择了更多包含 RTX 的治疗方案。
在治疗难治性 LN 或 LN 复发方面,儿科风湿病学家和肾脏病学家的治疗选择差异很大,风湿病学家更常选择利妥昔单抗。需要进一步研究以阐明这一发现背后的原因。本研究强调了在制定儿童 LN 共识治疗方案方面开展合作努力的重要性。