Torres Irene, Thapa Bishnu, Robbins Grace, Koya Shaffi Fazaludeen, Abdalla Salma M, Arah Onyebuchi A, Weeks William B, Zhang Luxia, Asma Samira, Morales Jeanette Vega, Galea Sandro, Larson Heidi J, Rhee Kyu
Fundacion Octaedro, Quito, Ecuador.
Rockefeller Foundation-Boston University 3-D Commission on Determinants, Data, and Decision-making, Boston, USA.
J Urban Health. 2021 Aug;98(Suppl 1):31-40. doi: 10.1007/s11524-021-00558-7. Epub 2021 Sep 1.
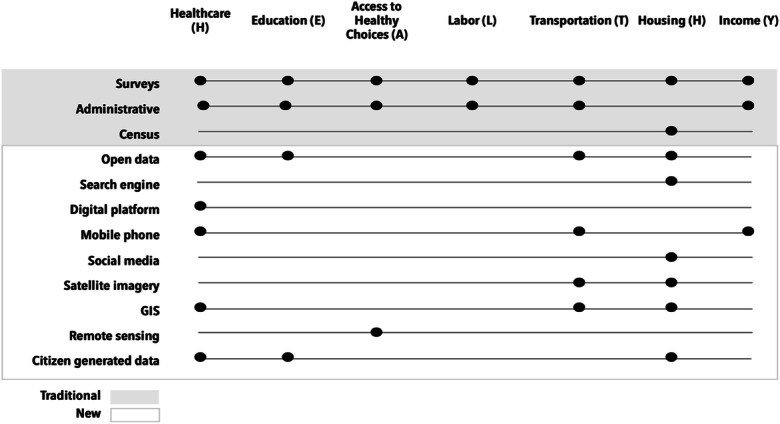
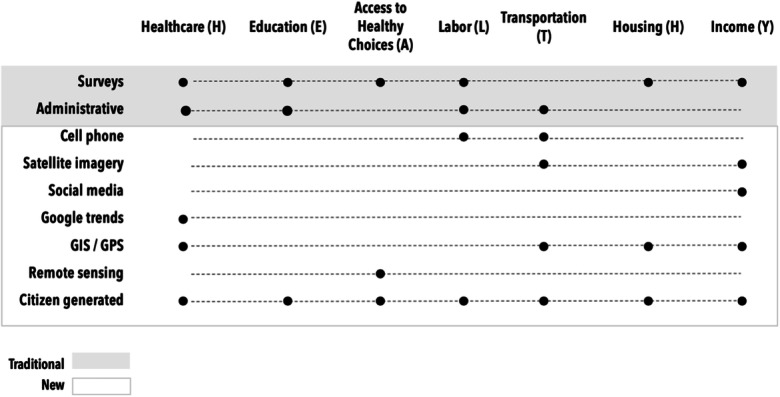
The expansion in the scope, scale, and sources of data on the wider social determinants of health (SDH) in the last decades could bridge gaps in information available for decision-making. However, challenges remain in making data widely available, accessible, and useful towards improving population health. While traditional, government-supported data sources and comparable data are most often used to characterize social determinants, there are still capacity and management constraints on data availability and use. Conversely, privately held data may not be shared. This study reviews and discusses the nature, sources, and uses of data on SDH, with illustrations from two middle-income countries: Kenya and the Philippines. The review highlights opportunities presented by new data sources, including the use of big data technologies, to capture data on social determinants that can be useful to inform population health. We conducted a search between October 2010 and September 2020 for grey and scientific publications on social determinants using a search strategy in PubMed and a manual snowball search. We assessed data sources and the data environment in both Kenya and the Philippines. We found limited evidence of the use of new sources of data to study the wider SDH, as most of the studies available used traditional sources. There was also no evidence of qualitative big data being used. Kenya has more publications using new data sources, except on the labor determinant, than the Philippines. The Philippines has a more consistent distribution of the use of new data sources across the HEALTHY determinants than Kenya, where there is greater variation of the number of publications across determinants. The results suggest that both countries use limited SDH data from new data sources. This limited use could be due to a number of factors including the absence of standardized indicators of SDH, inadequate trust and acceptability of data collection methods, and limited infrastructure to pool, analyze, and translate data.
在过去几十年里,关于健康的更广泛社会决定因素(SDH)的数据在范围、规模和来源上的扩展,可能会弥合决策可用信息方面的差距。然而,在使数据广泛可用、可获取并有助于改善人群健康方面,挑战依然存在。虽然传统的、政府支持的数据源和可比数据最常被用于描述社会决定因素,但在数据的可用性和使用方面仍存在能力和管理限制。相反,私有数据可能不会被共享。本研究回顾并讨论了SDH数据的性质、来源和用途,并以两个中等收入国家肯尼亚和菲律宾为例进行说明。该回顾强调了新数据源带来的机遇,包括使用大数据技术来获取对人群健康有益的社会决定因素数据。我们在2010年10月至2020年9月期间,使用PubMed中的搜索策略和手动滚雪球搜索法,搜索了关于社会决定因素的灰色文献和科学出版物。我们评估了肯尼亚和菲律宾的数据来源及数据环境。我们发现,使用新数据源研究更广泛的SDH的证据有限,因为现有大多数研究使用的是传统来源。也没有定性大数据被使用的证据。与菲律宾相比,肯尼亚除了在劳动力决定因素方面外,使用新数据源的出版物更多。菲律宾在各健康决定因素中使用新数据源的分布比肯尼亚更一致,而肯尼亚各决定因素的出版物数量差异更大。结果表明,两国都使用来自新数据源的有限的SDH数据。这种有限的使用可能是由于多种因素造成的,包括缺乏SDH的标准化指标、数据收集方法的信任度和可接受性不足,以及汇总、分析和转化数据的基础设施有限。