Great Ormond Street Institute of Child Health, University College London, London, United Kingdom.
Department of Pediatrics and Adolescent Medicine, Aarhus University Hospital, Aarhus, Denmark.
Front Immunol. 2021 Jul 29;12:643189. doi: 10.3389/fimmu.2021.643189. eCollection 2021.
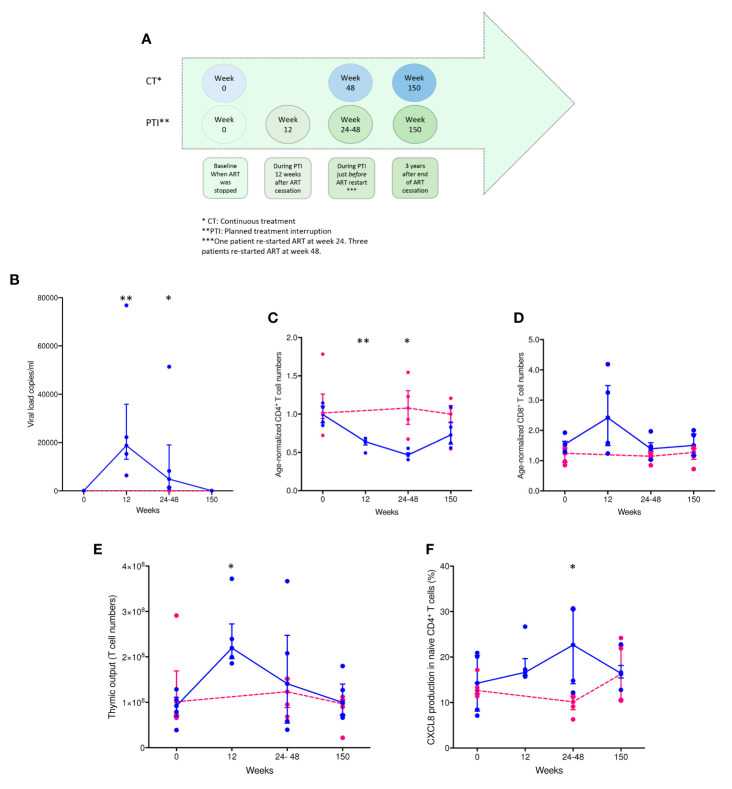
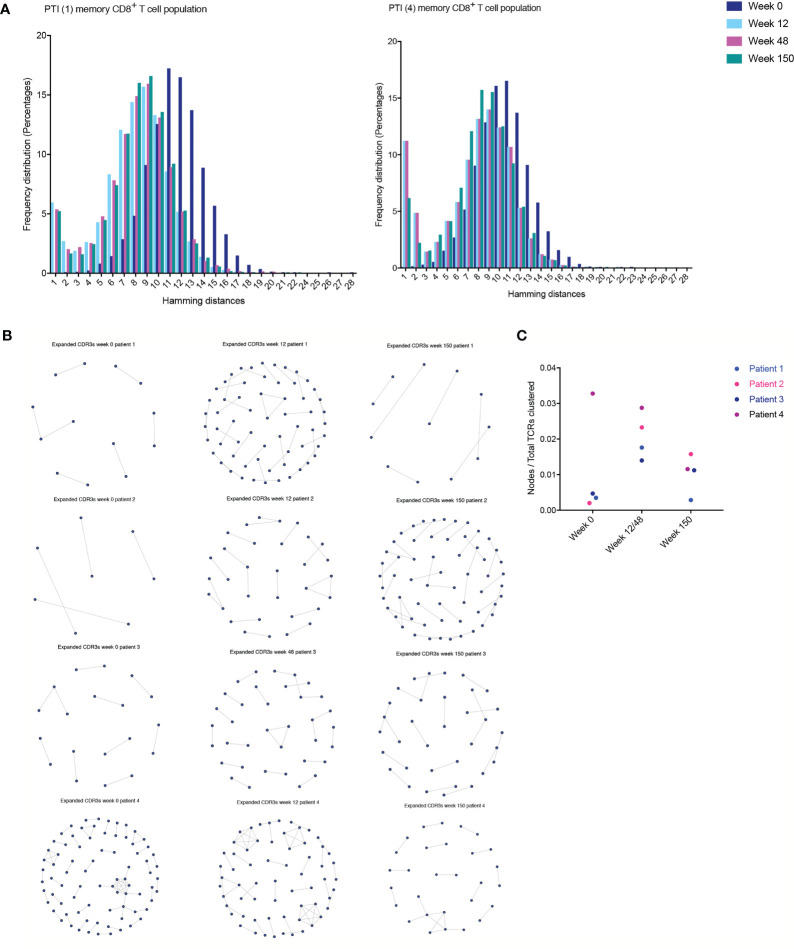
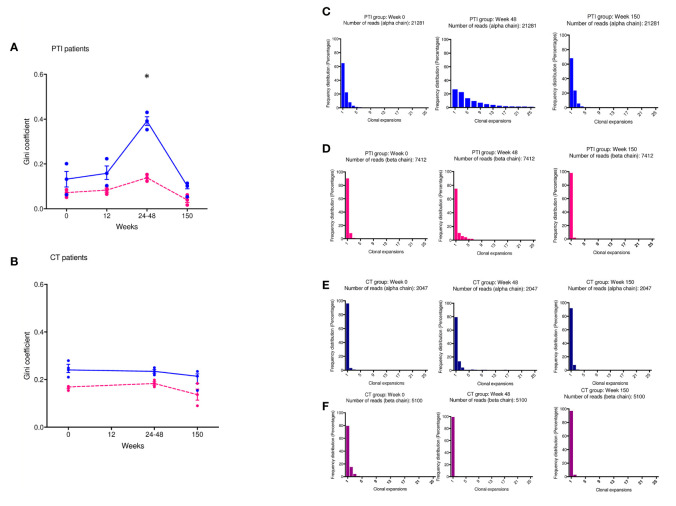
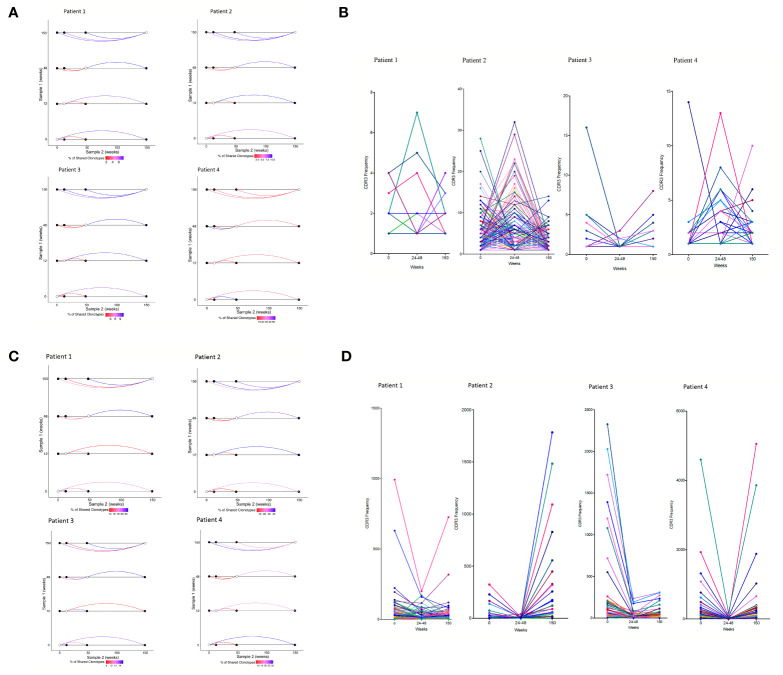
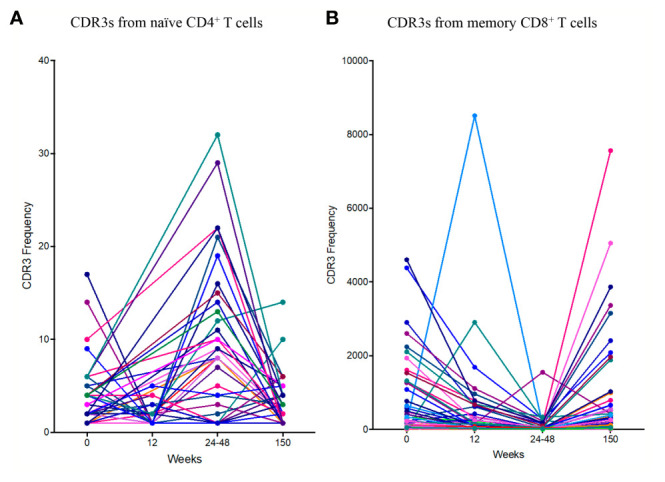
It is intriguing that, unlike adults with HIV-1, children with HIV-1 reach a greater CD4 T cell recovery following planned treatment cessation. The reasons for the better outcomes in children remain unknown but may be related to increased thymic output and diversity of T cell receptor repertoires. HIV-1 infected children from the PENTA 11 trial tolerated planned treatment interruption without adverse long-term clinical, virological, or immunological consequences, once antiretroviral therapy was re-introduced. This contrasts to treatment interruption trials of HIV-1 infected adults, who had rapid changes in T cells and slow recovery when antiretroviral therapy was restarted. How children can develop such effective immune responses to planned treatment interruption may be critical for future studies. PENTA 11 was a randomized, phase II trial of planned treatment interruptions in HIV-1-infected children (ISRCTN 36694210). In this sub-study, eight patients in long-term follow-up were chosen with CD4 count>500/ml, viral load <50c/ml at baseline: four patients on treatment interruption and four on continuous treatment. Together with measurements of thymic output, we used high-throughput next generation sequencing and bioinformatics to systematically organize memory CD8 and naïve CD4 T cell receptors according to diversity, clonal expansions, sequence sharing, antigen specificity, and T cell receptor similarities following treatment interruption compared to continuous treatment. We observed an increase in thymic output following treatment interruption compared to continuous treatment. This was accompanied by an increase in T cell receptor clonal expansions, increased T cell receptor sharing, and higher sequence similarities between patients, suggesting a more focused T cell receptor repertoire. The low numbers of patients included is a limitation and the data should be interpreted with caution. Nonetheless, the high levels of thymic output and the high diversity of the T cell receptor repertoire in children may be sufficient to reconstitute the T cell immune repertoire and reverse the impact of interruption of antiretroviral therapy. Importantly, the effective T cell receptor repertoires following treatment interruption may inform novel therapeutic strategies in children infected with HIV-1.
有趣的是,与感染 HIV-1 的成年人不同,计划停止治疗后,儿童的 CD4 T 细胞恢复得更多。儿童的结果更好的原因尚不清楚,但可能与胸腺输出增加和 T 细胞受体库多样性有关。在 PENTA 11 试验中,感染 HIV-1 的儿童在停止计划治疗后,一旦重新开始抗逆转录病毒治疗,没有出现不良的长期临床、病毒学或免疫学后果,能够耐受计划的治疗中断。这与感染 HIV-1 的成年人的治疗中断试验形成对比,后者在重新开始抗逆转录病毒治疗时,T 细胞迅速变化,恢复缓慢。儿童如何对计划的治疗中断产生如此有效的免疫反应,这可能对未来的研究至关重要。PENTA 11 是一项针对 HIV-1 感染儿童的计划治疗中断的随机、二期试验(ISRCTN 36694210)。在这项子研究中,选择了长期随访中 CD4 计数>500/ml、基线时病毒载量<50c/ml 的 8 名患者:4 名患者接受治疗中断,4 名患者接受持续治疗。除了测量胸腺输出外,我们还使用高通量下一代测序和生物信息学,根据治疗中断与持续治疗相比的多样性、克隆扩增、序列共享、抗原特异性和 T 细胞受体相似性,系统地组织记忆 CD8 和幼稚 CD4 T 细胞受体。与持续治疗相比,我们观察到治疗中断后胸腺输出增加。这伴随着 T 细胞受体克隆扩增增加、T 细胞受体共享增加以及患者之间的序列相似性增加,表明 T 细胞受体库更加集中。纳入的患者数量较少是一个限制,数据应谨慎解释。尽管如此,儿童中较高的胸腺输出水平和 T 细胞受体库的高度多样性可能足以重建 T 细胞免疫库并逆转抗逆转录病毒治疗中断的影响。重要的是,治疗中断后有效的 T 细胞受体库可能为感染 HIV-1 的儿童提供新的治疗策略信息。