Department of Cardiology Amsterdam Cardiovascular Sciences (ACS) Amsterdam UMC, Vrije Universiteit Amsterdam Amsterdam The Netherlands.
Department of Pulmonology Amsterdam Cardiovascular Sciences (ACS) Amsterdam UMC, Vrije Universiteit Amsterdam Amsterdam The Netherlands.
J Am Heart Assoc. 2021 Sep 21;10(18):e021165. doi: 10.1161/JAHA.121.021165. Epub 2021 Sep 3.
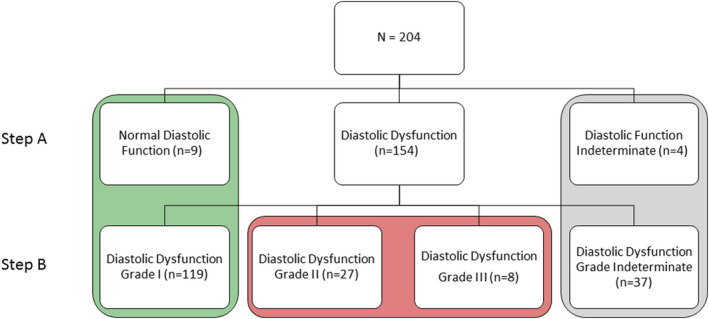
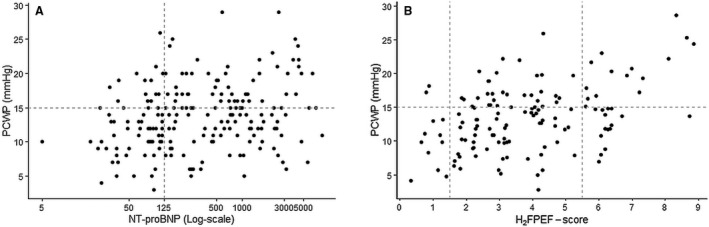
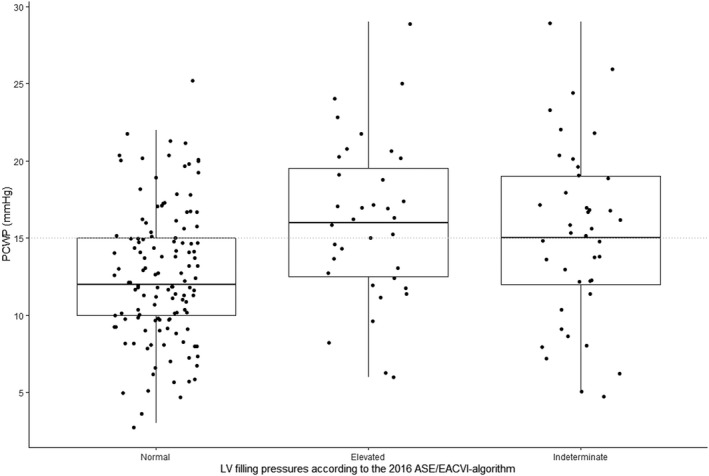
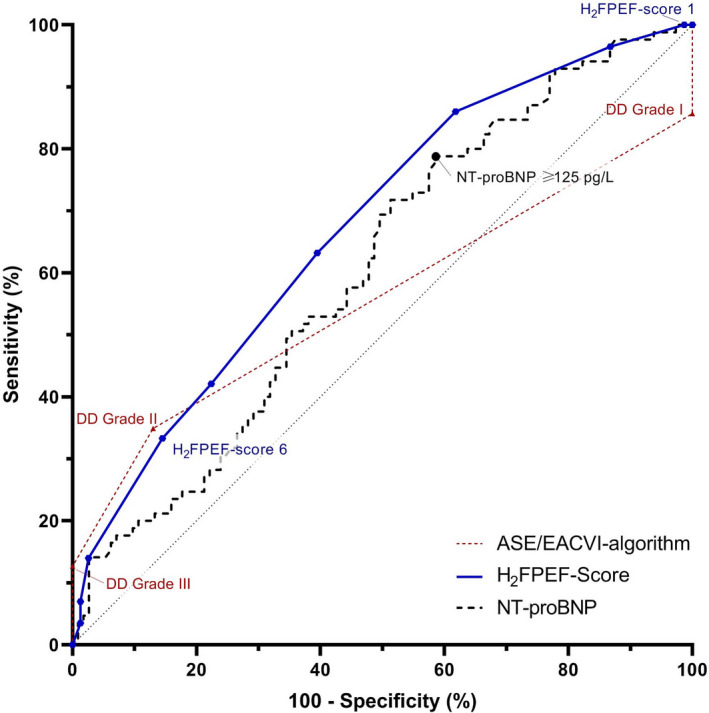
Background Echocardiography is considered the cornerstone of the diagnostic workup of heart failure with preserved ejection fraction. Thus far, validation of the 2016 American Society of Echocardiography/European Association of Cardiovascular Imaging (ASE/EACVI) echo-algorithm for evaluation of diastolic (dys)function in a patient suspected of heart failure with preserved ejection fraction has been limited. Methods and Results The diagnostic performance of the 2016 ASE/EACVI algorithm was assessed in 204 patients evaluated for unexplained dyspnea or pulmonary hypertension with echocardiogram and right heart catheterization. Invasively measured pulmonary capillary wedge pressure (PCWP) was used as the gold standard. In addition, the diagnostic performance of HFPEF score and NT-proBNP (N-terminal pro-B-type natriuretic peptide) were evaluated. There was a poor correlation between indexed left atrial volume, E/e' (septal and average) or early mitral inflow (E), and PCWP (=0.25-0.30, values all <0.01). No correlation was found in our cohort between e' (septal or lateral) or tricuspid valve regurgitation and PCWP. The correlation between diastolic function grades of the ASE/EACVI algorithm and PCWP was poor (=0.17, <0.05). The ASE/EACVI algorithm had a sensitivity and specificity of 35% and 87%, respectively; an accuracy of 67% and an area under the curve of 0.56. Moreover, in 30% of cases the algorithm was not applicable or indeterminate. HFPEF score had a modest correlation with PCWP (=0.44, <0.0001), and accuracy was 73%; NT-proBNP correlated weakly with PCWP (=0.24, <0.001), and accuracy was 57%. Conclusions The 2016 ASE/EACVI algorithm for the assessment of diastolic function has a limited diagnostic accuracy in patients evaluated for unexplained dyspnea and/or pulmonary hypertension, and especially sensitivity to detect diastolic dysfunction was low.
背景 超声心动图被认为是射血分数保留心力衰竭诊断工作的基石。迄今为止,2016 年美国超声心动图学会/欧洲心血管影像协会(ASE/EACVI)评估舒张功能障碍的超声算法在射血分数保留心力衰竭患者中的验证是有限的。
方法和结果 我们评估了 204 例因不明原因呼吸困难或肺动脉高压而行超声心动图和右心导管检查的患者中,2016 年 ASE/EACVI 算法的诊断性能。采用有创性测量的肺毛细血管楔压(PCWP)作为金标准。此外,还评估了 HFPEF 评分和 NT-proBNP(N 端脑利钠肽前体)的诊断性能。左心房容积指数、E/e'(间隔和平均)或早期二尖瓣流入(E)与 PCWP 之间相关性差(=0.25-0.30, 值均<0.01)。在我们的队列中,没有发现 e'(间隔或侧壁)或三尖瓣反流与 PCWP 之间的相关性。ASE/EACVI 算法的舒张功能分级与 PCWP 的相关性较差(=0.17,<0.05)。ASE/EACVI 算法的敏感性和特异性分别为 35%和 87%;准确性为 67%,曲线下面积为 0.56。此外,在 30%的病例中,该算法不可用或不确定。HFPEF 评分与 PCWP 有中度相关性(=0.44,<0.0001),准确性为 73%;NT-proBNP 与 PCWP 弱相关(=0.24,<0.001),准确性为 57%。
结论 在评估不明原因呼吸困难和/或肺动脉高压的患者中,2016 年 ASE/EACVI 评估舒张功能的算法诊断准确性有限,特别是检测舒张功能障碍的敏感性较低。