Kist Janet M, Smit Gideon W G, Mairuhu Albert T A, Struijs Jeroen N, Vos Rimke C, van Peet Petra G, Vos Hedwig M M, Beishuizen Edith D, Sijpkens Yvo W J, Groenwold Rolf H H, Numans Mattijs E
Department of Public Health & Primary Care, Leiden University Medical Center, Campus The Hague, the Netherlands.
Department of Internal Medicine, HAGA Teaching Hospital, The Hague, the Netherlands.
EClinicalMedicine. 2021 Aug 29;40:101120. doi: 10.1016/j.eclinm.2021.101120. eCollection 2021 Oct.
Socioeconomic status and ethnicity are not incorporated as predictors in country-level cardiovascular risk charts on mainland Europe. The aim of this study was to quantify the sex-specific cardiovascular death rates stratified by ethnicity and socioeconomic factors in an urban population in a universal healthcare system.
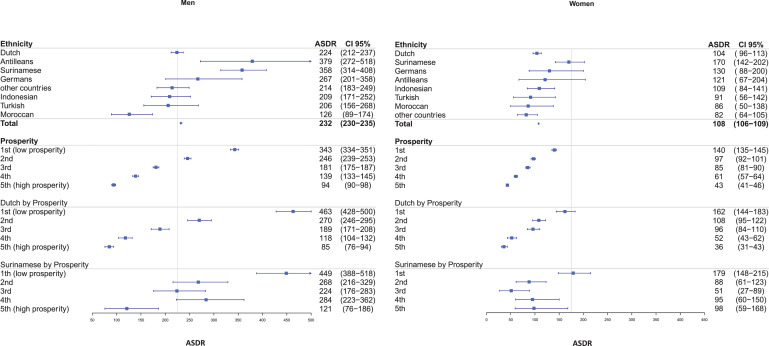
Age-standardized death rates (ASDR) were estimated in a dynamic population, aged 45-75 in the city of The Hague, the Netherlands, over the period 2007-2018, using data of Statistics Netherlands. Results were stratified by sex, ethnicity (country of birth) and socioeconomic status (prosperity) and compared with a European cut-off for high-risk countries (ASDR men 225/100,000 and women 175/100,000).
In total, 3073 CVD deaths occurred during 1·76 million person years follow-up. Estimated ASDRs (selected countries of birth) ranged from 126 (95%CI 89-174) in Moroccan men to 379 (95%CI 272-518) in Antillean men, and from 86 (95%CI 50-138) in Moroccan women to 170 (95%CI 142-202) in Surinamese women. ASDRs in the highest and lowest prosperity quintiles were 94 (95%CI 90-98) and 343 (95%CI 334-351) for men, and 43 (95%CI 41-46) and 140 (95%CI 135-145), for women, respectively.
In a diverse urban population, large health disparities in cardiovascular ASDRs exists across ethnic and socioeconomic subgroups. Identifying these high-risk subgroups followed by targeted preventive efforts, might provide a basis for improving cardiovascular health equity within communities. Instead of classifying countries as high-risk or low-risk, a shift towards focusing on these subgroups within countries might be needed.
Leiden University Medical Center and Leiden University.
在欧洲大陆的国家层面心血管风险图表中,社会经济地位和种族并未被纳入预测因素。本研究的目的是在一个全民医疗体系的城市人口中,按种族和社会经济因素对特定性别的心血管死亡率进行量化。
利用荷兰统计局的数据,对2007年至2018年期间荷兰海牙市45至75岁的动态人群的年龄标准化死亡率(ASDR)进行了估计。结果按性别、种族(出生国)和社会经济地位(繁荣程度)进行分层,并与欧洲高风险国家的临界值(男性ASDR为225/10万,女性为175/10万)进行比较。
在176万人年的随访期间,共发生了3073例心血管疾病死亡。估计的ASDR(选定的出生国)范围从摩洛哥男性的126(95%CI 89-174)到安的列斯男性的379(95%CI 272-518),以及从摩洛哥女性的86(95%CI 50-138)到苏里南女性的170(95%CI 142-202)。最高和最低繁荣五分位数的男性ASDR分别为94(95%CI 90-98)和343(95%CI 334-351),女性分别为43(95%CI 41-46)和140(95%CI 135-145)。
在一个多样化的城市人口中,心血管ASDR在种族和社会经济亚组之间存在巨大的健康差异。识别这些高风险亚组并随后进行有针对性的预防措施,可能为改善社区内的心血管健康公平性提供基础。与其将国家分类为高风险或低风险,可能需要转向关注国家内部的这些亚组。
莱顿大学医学中心和莱顿大学。