Centre for Diet and Activity Research, Medical Research Council (MRC) Epidemiology Unit, Institute of Metabolic Science, Cambridge Biomedical Campus, University of Cambridge School of Clinical Medicine, Box 285, Cambridge, CB2 0QQ, UK.
Amsterdam UMC, University of Amsterdam Department of Public Health, Amsterdam Public Health Institute, Meibergdreef 9, 1105 AZ, Amsterdam, The Netherlands.
Eur J Clin Nutr. 2020 Mar;74(3):387-396. doi: 10.1038/s41430-019-0463-4. Epub 2019 Jul 10.
BACKGROUND/OBJECTIVES: Socioeconomic inequalities in diet quality are consistently reported, but few studies have investigated whether and how such inequalities vary across ethnic groups. This study aimed to examine differences in diet quality and socioeconomic patterning of diet quality across ethnic groups.
SUBJECTS/METHODS: Cross-sectional data from the HELIUS study were used. Dutch, South-Asian Surinamese, African Surinamese, Ghanaian, Turkish and Moroccan adults (aged 18-70 years) were randomly sampled, stratified by ethnicity. Dietary intake was estimated among a subsample (n = 4602) from 200-item, ethnic-specific food frequency questionnaires, and diet quality was assessed using the Dutch Healthy Diet Index 2015 (DHD15-Index). Wald tests were used to compare non-Dutch and Dutch participants. Adjusted linear regression models were used to examine differences in DHD15-Index by three indicators of socioeconomic position: educational level, occupational status and perceived financial difficulties. All analyses were stratified by sex.
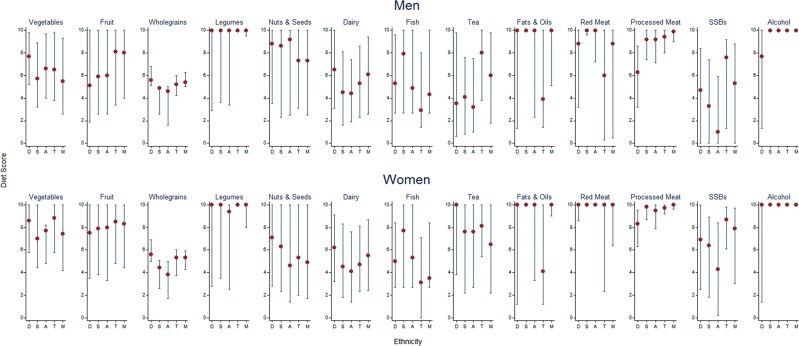
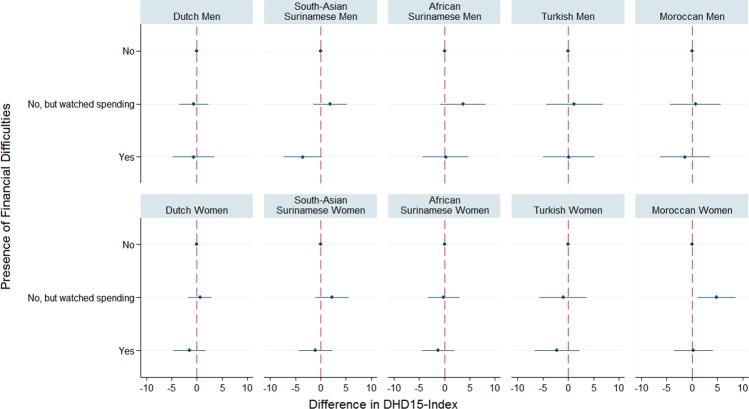
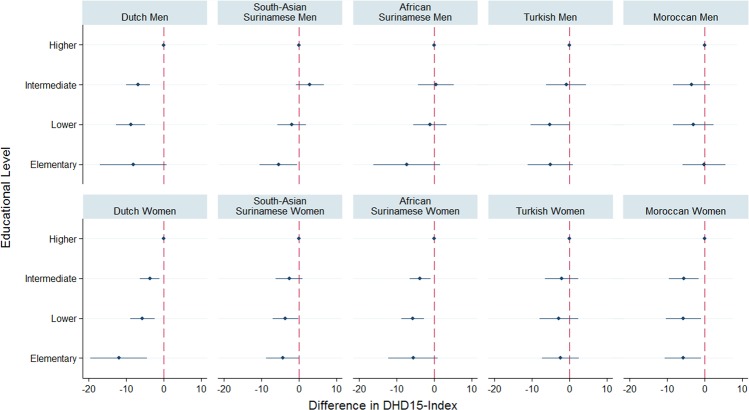
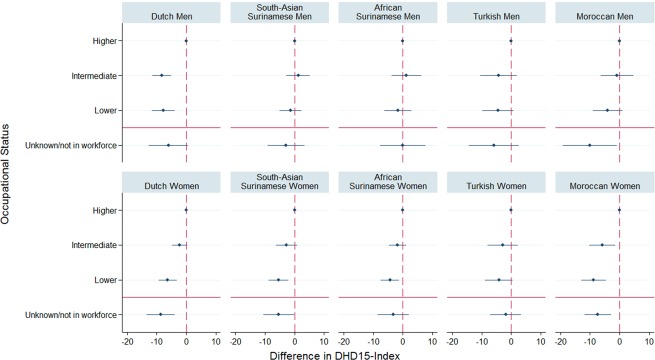
Dutch participants had lower median DHD15-Index than most ethnic minority participants (P < 0.001). Lower educational level was associated with lower DHD15-Index among Dutch men (P < 0.0001), South-Asian Surinamese men (P = 0.01), Dutch women (P = 0.0001), African Surinamese women (P = 0.002) and Moroccan women (P = 0.04). Lower occupational status was associated with lower DHD15-Index in Dutch men, β -7.8 (95% CI -11.7, -3.9) and all women (β -4.4 to -8.8), except Turkish women. DHD15-Index was not associated with perceived financial difficulties in most groups.
We observed variations in diet quality across ethnic groups. Low socioeconomic position was not consistently associated with poor diet quality in all ethnic groups. This may be due to ethnicity-specific retention of traditional diets, irrespective of socioeconomic position.
背景/目的:社会经济不平等与饮食质量有关,这一点已得到广泛报道,但很少有研究调查这种不平等在不同族裔群体中是否存在以及如何存在差异。本研究旨在研究不同族裔群体之间饮食质量的差异以及饮食质量的社会经济模式。
受试者/方法:本研究使用了 HELIUS 研究的横断面数据。荷兰人、南亚苏里南人、非裔苏里南人、加纳人、土耳其人和摩洛哥成年人(年龄在 18-70 岁之间)按族裔进行分层随机抽样。在 200 项特定族裔的食物频率问卷的子样本(n=4602)中估计了饮食摄入量,并使用 2015 年荷兰健康饮食指数(DHD15-Index)评估了饮食质量。使用 Wald 检验比较了非荷兰人和荷兰参与者。使用调整后的线性回归模型,根据三个社会经济地位指标(教育水平、职业地位和感知经济困难),检验了 DHD15-Index 的差异。所有分析均按性别分层。
与大多数少数族裔参与者相比,荷兰参与者的 DHD15-Index 中位数较低(P<0.001)。较低的教育水平与荷兰男性(P<0.0001)、南亚苏里南男性(P=0.01)、荷兰女性(P=0.0001)、非裔苏里南女性(P=0.002)和摩洛哥女性(P=0.04)的 DHD15-Index 较低相关。较低的职业地位与荷兰男性(β-7.8[95%CI-11.7,-3.9]和所有女性(β-4.4 至-8.8),除了土耳其女性)的 DHD15-Index 较低相关。在大多数群体中,DHD15-Index 与感知经济困难无关。
我们观察到不同族裔群体之间的饮食质量存在差异。在所有族裔群体中,低社会经济地位并不总是与不良饮食质量相关。这可能是由于特定族裔保留了传统饮食,而不论社会经济地位如何。