Department of Pathology, University Clermont Auvergne, INSERM U1240, Centre Jean Perrin, Clermont-Ferrand, France.
Department of Pathology, University Clermont Auvergne, INSERM U1240, Centre Jean Perrin, Clermont-Ferrand, France.
ESMO Open. 2021 Oct;6(5):100257. doi: 10.1016/j.esmoop.2021.100257. Epub 2021 Sep 3.
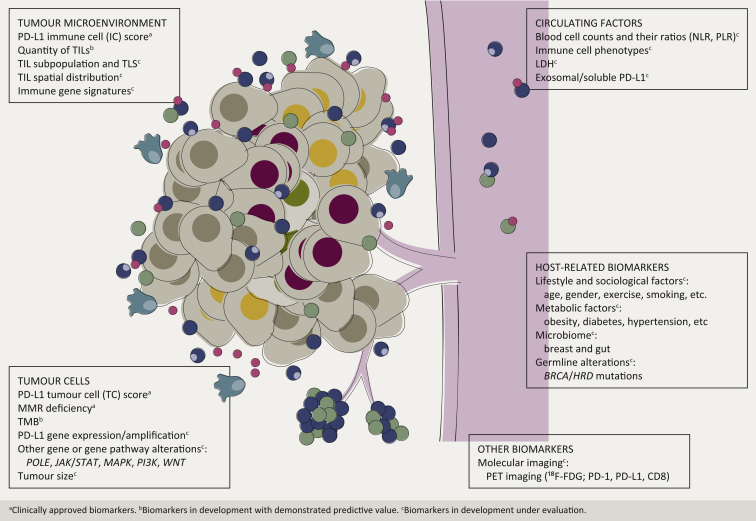
Therapies that modulate immune response to cancer, such as immune checkpoint inhibitors, began an intense development a few years ago; however, in breast cancer (BC), the results have been relatively disappointing so far. Finding biomarkers for better selection of BC patients for various immunotherapies remains a significant unmet medical need. At present, only tumour tissue programmed death-ligand 1 (PD-L1) and mismatch repair deficiency status are approved as theranostic biomarkers for programmed cell death-1 (PD-1)/PD-L1 inhibitors in BC. However, due to the complexity of tumour microenvironment (TME) and cancer response to immunomodulators, none of them is a perfect selector. Therefore, an intense quest is ongoing for complementary tumour- or host-related predictive biomarkers in breast immuno-oncology. Among the upcoming biomarkers, quantity, immunophenotype and spatial distribution of tumour-infiltrating lymphocytes and other TME cells as well as immune gene signatures emerge as most promising and are being increasingly tested in clinical trials. Biomarkers or strategies allowing dynamic assessment of BC response to immunotherapy, such as circulating/exosomal PD-L1, quantity of white/immune blood cell subpopulations and molecular imaging are particularly suitable for immunotreatment monitoring. Finally, host-related factors, such as microbiome and lifestyle, should also be taken into account when planning integration of immunomodulating therapies into BC management. As none of the biomarkers taken separately is accurate enough, the solution could come from composite biomarkers, which would combine clinical, molecular and immunological features of the disease, possibly powered by artificial intelligence.
近年来,能够调节癌症免疫反应的疗法(如免疫检查点抑制剂)得到了迅猛发展;然而,迄今为止,这些疗法在乳腺癌(BC)中的应用效果仍相对令人失望。寻找生物标志物以更好地选择适合各种免疫疗法的 BC 患者,仍然是一个重大的未满足的医疗需求。目前,只有肿瘤组织程序性死亡配体 1(PD-L1)和错配修复缺陷状态被批准为 BC 中程序性细胞死亡-1(PD-1)/PD-L1 抑制剂的治疗诊断生物标志物。然而,由于肿瘤微环境(TME)的复杂性和癌症对免疫调节剂的反应,这些标志物都不是完美的选择器。因此,人们正在积极寻找补充性的与肿瘤或宿主相关的预测性生物标志物,用于乳腺癌免疫肿瘤学。在即将出现的生物标志物中,肿瘤浸润淋巴细胞和其他 TME 细胞的数量、免疫表型和空间分布以及免疫基因特征被认为是最有前途的,并在临床试验中得到了越来越多的测试。能够动态评估 BC 对免疫治疗反应的生物标志物或策略,如循环/外泌体 PD-L1、白细胞/免疫细胞亚群的数量以及分子成像,特别适合免疫治疗监测。最后,在规划将免疫调节疗法纳入 BC 管理时,还应考虑宿主相关因素,如微生物组和生活方式。由于单独使用任何一种生物标志物都不够准确,因此解决方案可能来自于复合生物标志物,它将结合疾病的临床、分子和免疫学特征,可能由人工智能提供支持。