Department of Cardiovascular Medicine, Cleveland Clinic, Cleveland, Ohio, USA.
Department of Cardiovascular Medicine, Toho University Faculty of Medicine, Ota-ku, Japan.
BMJ Open. 2021 Sep 8;11(9):e052708. doi: 10.1136/bmjopen-2021-052708.
Predictive algorithms to inform risk management decisions are needed for patients with COVID-19, although the traditional risk scores have not been adequately assessed in Asian patients. We aimed to evaluate the performance of a COVID-19-specific prediction model, the 4C (Coronavirus Clinical Characterisation Consortium) Mortality Score, along with other conventional critical care risk models in Japanese nationwide registry data.
Retrospective cohort study.
Hospitalised patients with COVID-19 and cardiovascular disease or coronary risk factors from January to May 2020 in 49 hospitals in Japan.
Two different types of outcomes, in-hospital mortality and a composite outcome, defined as the need for invasive mechanical ventilation and mortality.
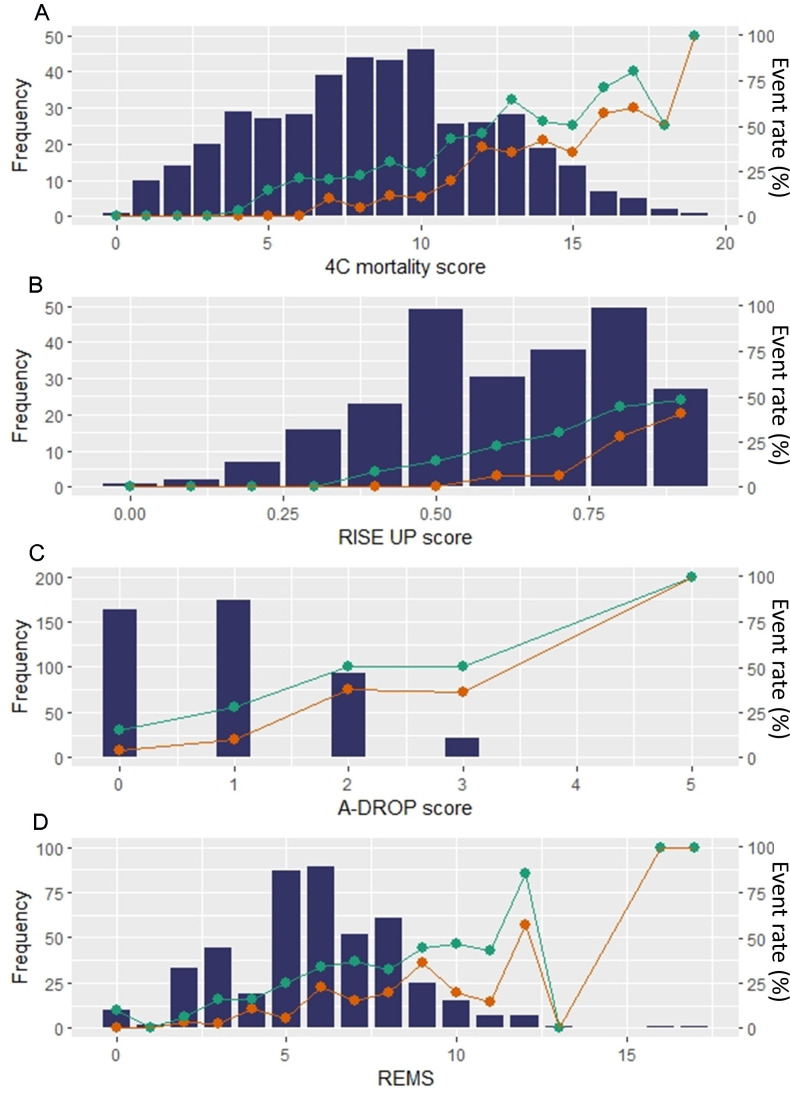
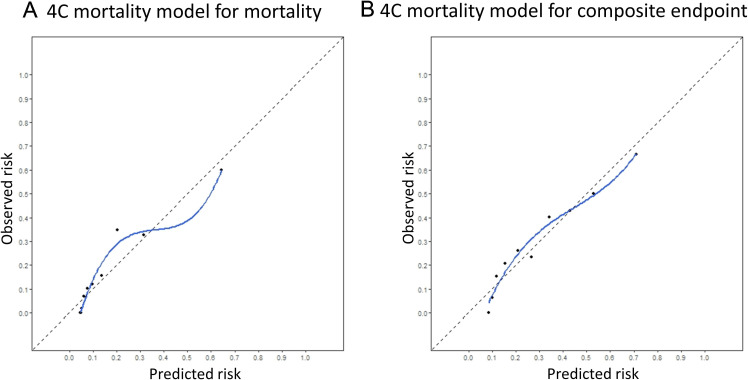
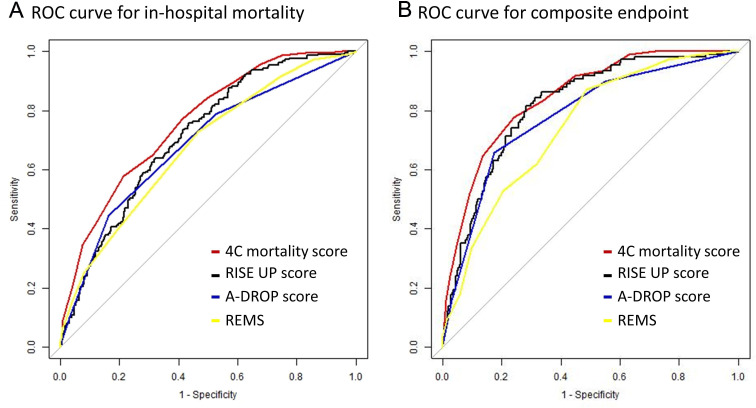
The risk scores for 693 patients were tested by predicting in-hospital mortality for all patients and composite endpoint among those not intubated at baseline (n=659). The number of events was 108 (15.6%) for mortality and 178 (27.0%) for composite endpoints. After missing values were multiply imputed, the performance of the 4C Mortality Score was assessed and compared with three prediction models that have shown good discriminatory ability (RISE UP score, A-DROP score and the Rapid Emergency Medicine Score (REMS)). The area under the receiver operating characteristic curve (AUC) for the 4C Mortality Score was 0.84 (95% CI 0.80 to 0.88) for in-hospital mortality and 0.78 (95% CI 0.74 to 0.81) for the composite endpoint. It showed greater discriminatory ability compared with other scores, except for the RISE UP score, for predicting in-hospital mortality (AUC: 0.82, 95% CI 0.78 to 0.86). Similarly, the 4C Mortality Score showed a positive net reclassification improvement index over the A-DROP and REMS for mortality and over all three scores for the composite endpoint. The 4C Mortality Score model showed good calibration, regardless of outcome.
The 4C Mortality Score performed well in an independent external COVID-19 cohort and may enable appropriate disposition of patients and allocation of medical resources. UMIN000040598.
对于 COVID-19 患者,需要预测风险的算法来辅助决策,但传统的风险评分在亚洲患者中尚未得到充分评估。我们旨在评估 COVID-19 特异性预测模型 4C(冠状病毒临床特征联盟)死亡率评分,以及其他常规重症监护风险模型在日本全国登记数据中的表现。
回顾性队列研究。
2020 年 1 月至 5 月,日本 49 家医院收治的 COVID-19 合并心血管疾病或冠心病危险因素的住院患者。
两种不同的结局,住院死亡率和复合结局(定义为需要有创机械通气和死亡)。
对 693 例患者的风险评分进行了测试,用于预测所有患者的住院死亡率和基线时未插管患者的复合终点(n=659)。死亡率的事件数为 108 例(15.6%),复合终点为 178 例(27.0%)。在对缺失值进行多次插补后,评估了 4C 死亡率评分的性能,并与三个具有良好区分能力的预测模型(RISE UP 评分、A-DROP 评分和快速急诊医学评分(REMS))进行了比较。4C 死亡率评分对住院死亡率的接收者操作特征曲线下面积(AUC)为 0.84(95%CI 0.80 至 0.88),对复合终点的 AUC 为 0.78(95%CI 0.74 至 0.81)。与其他评分相比,除 RISE UP 评分外,该评分在预测住院死亡率方面具有更好的区分能力(AUC:0.82,95%CI 0.78 至 0.86)。同样,4C 死亡率评分在死亡率方面显示出对 A-DROP 和 REMS 的正净重新分类改善指数,在复合终点方面显示出对所有三个评分的正净重新分类改善指数。4C 死亡率评分模型表现出良好的校准能力,与结局无关。
4C 死亡率评分在独立的 COVID-19 外部队列中表现良好,可能有助于对患者进行适当的处置和医疗资源的分配。UMIN000040598。