Centre for Medical Informatics, The University of Edinburgh, Usher Institute of Population Health Sciences and Informatics, Edinburgh, UK.
University College London Institute for Global Health, London, UK.
Thorax. 2022 Jun;77(6):606-615. doi: 10.1136/thoraxjnl-2021-217629. Epub 2021 Nov 22.
To prospectively validate two risk scores to predict mortality (4C Mortality) and in-hospital deterioration (4C Deterioration) among adults hospitalised with COVID-19.
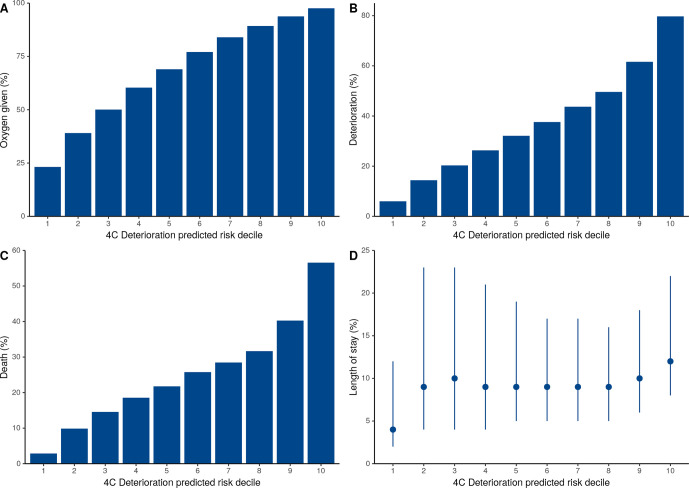
Prospective observational cohort study of adults (age ≥18 years) with confirmed or highly suspected COVID-19 recruited into the International Severe Acute Respiratory and emerging Infections Consortium (ISARIC) WHO Clinical Characterisation Protocol UK (CCP-UK) study in 306 hospitals across England, Scotland and Wales. Patients were recruited between 27 August 2020 and 17 February 2021, with at least 4 weeks follow-up before final data extraction. The main outcome measures were discrimination and calibration of models for in-hospital deterioration (defined as any requirement of ventilatory support or critical care, or death) and mortality, incorporating predefined subgroups.
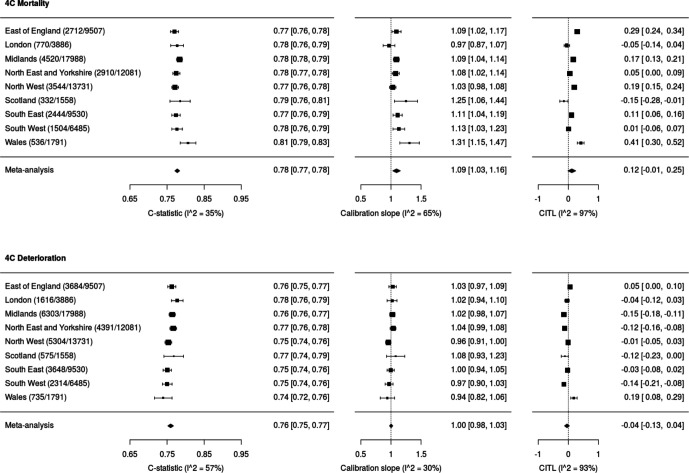
76 588 participants were included, of whom 27 352 (37.4%) deteriorated and 12 581 (17.4%) died. Both the 4C Mortality (0.78 (0.77 to 0.78)) and 4C Deterioration scores (pooled C-statistic 0.76 (95% CI 0.75 to 0.77)) demonstrated consistent discrimination across all nine National Health Service regions, with similar performance metrics to the original validation cohorts. Calibration remained stable (4C Mortality: pooled slope 1.09, pooled calibration-in-the-large 0.12; 4C Deterioration: 1.00, -0.04), with no need for temporal recalibration during the second UK pandemic wave of hospital admissions.
Both 4C risk stratification models demonstrate consistent performance to predict clinical deterioration and mortality in a large prospective second wave validation cohort of UK patients. Despite recent advances in the treatment and management of adults hospitalised with COVID-19, both scores can continue to inform clinical decision making.
ISRCTN66726260.
前瞻性验证两种风险评分模型,以预测因 COVID-19 住院的成年人的死亡率(4C 死亡率)和院内恶化(4C 恶化)。
前瞻性观察性队列研究纳入了年龄≥18 岁的成年人(成年人),他们在英格兰、苏格兰和威尔士的 306 家医院中参加了国际严重急性呼吸和新兴感染联合会(ISARIC)世界卫生组织临床特征化方案英国(CCP-UK)研究,这些成年人被确诊或高度疑似 COVID-19。患者于 2020 年 8 月 27 日至 2021 年 2 月 17 日期间入组,在最终数据提取前至少进行了 4 周的随访。主要结局指标为预测院内恶化(定义为任何通气支持或重症监护的需求,或死亡)和死亡率的模型的区分度和校准度,纳入了预定义的亚组。
共纳入 76588 名患者,其中 27352 名(37.4%)恶化,12581 名(17.4%)死亡。4C 死亡率评分(0.78(0.77 至 0.78))和 4C 恶化评分(汇总 C 统计量 0.76(95%CI 0.75 至 0.77))在所有 9 个国民保健服务地区均表现出一致的区分度,与原始验证队列的表现指标相似。校准仍然稳定(4C 死亡率:汇总斜率 1.09,汇总大范围校准 0.12;4C 恶化:1.00,-0.04),在英国第二波住院期间不需要进行时间校准。
4C 风险分层模型在英国患者的大规模前瞻性第二波验证队列中均表现出一致的预测临床恶化和死亡率的能力。尽管 COVID-19 住院成年患者的治疗和管理最近取得了进展,但这两个评分都可以继续为临床决策提供信息。
ISRCTN66726260。