Kim Jung Hyun, Lee Jae-Hoon, Lee Hye Sun, Shin Su-Jin, Park Eun Jung, Cho Eun-Suk, Baik Seung Hyuk, Lee Kang Young, Kang Jeonghyun
Department of Surgery, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Republic of Korea.
Department of Nuclear Medicine, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Republic of Korea.
J Inflamm Res. 2021 Sep 7;14:4457-4466. doi: 10.2147/JIR.S327443. eCollection 2021.
Recent data suggest that alterations in the neutrophil-to-lymphocyte ratio (NLR) in the perioperative periods can serve as prognostic factors. However, research on the clinical impact has been limited and even discordant in patients with colorectal cancer (CRC).
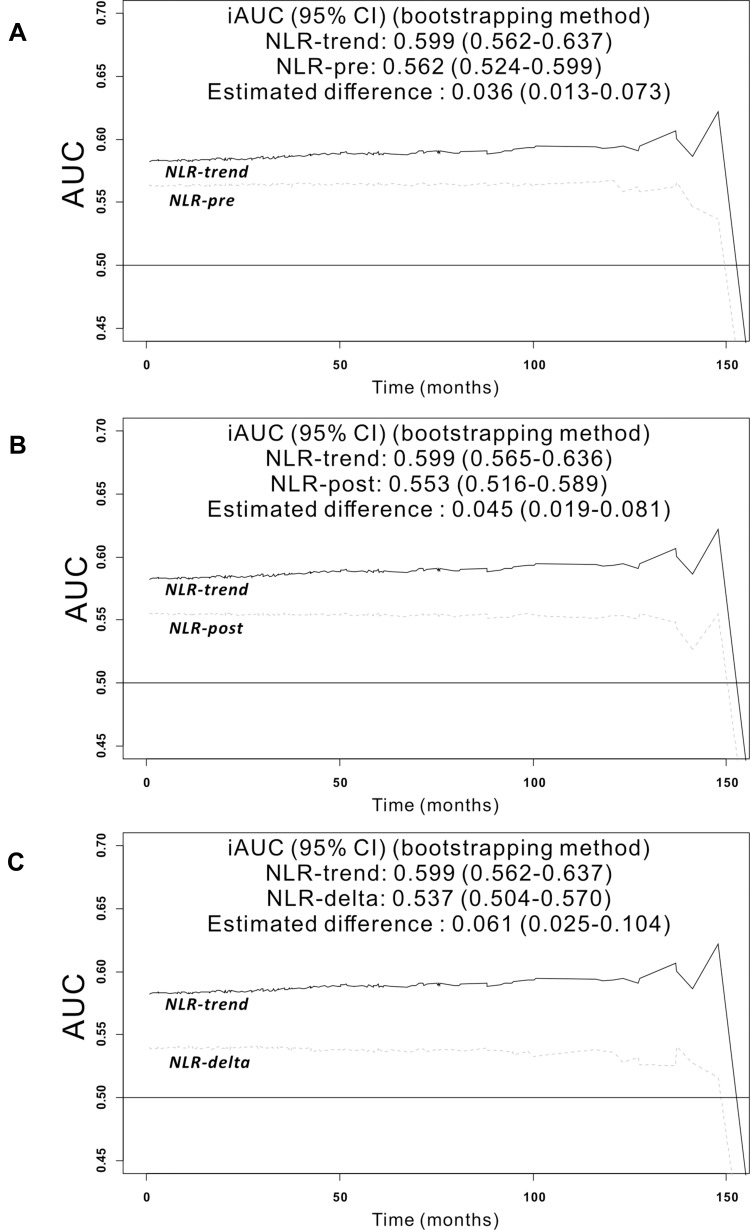
The optimal cut-off value of preoperative NLR (NLR-pre), postoperative NLR (NLR-post), and its change (NLR-delta) were determined to maximize differences in overall survival (OS) between groups. Patients were categorized into four groups (NLR-trend) as follows: G1, low NLR-pre and NLR-post; G2, low NLR-pre and high NLR-post; G3, high NLR-pre and low NLR-post; and G4, high NLR-pre and NLR-post. Discriminatory performance was compared using integrated AUC (iAUC) between all indicators.
A total of 576 patients diagnosed with stage I-IV CRC were included. The cut-off points were determined as 2.33 for NLR-pre, 2.06 for NLR-post, and -1.08 for NLR-delta. Subgroup dichotomization using NLR-pre, NLR-post, NLR-delta and NLR-trend were all identified as significant prognostic factors by univariate analysis. However, NLR-trend was only remained as an independent prognostic factor in the multivariate analysis. The iAUC of the NLR-trend was superior to that of NLR-pre (bootstrap iAUC mean difference=0.036; 95% CI 0.013-0.073), NLR-post (bootstrap iAUC mean difference=0.045; 95% CI 0.019-0.081) and NLR-delta (bootstrap iAUC mean difference=0.061; 95% CI 0.025-0.104).
Risk stratification and combining of preoperative and postoperative NLR (NLR-trend) can improve prognostic discrimination compared with single measurements or simple changes in NLR in patients with CRC.
近期数据表明,围手术期中性粒细胞与淋巴细胞比值(NLR)的改变可作为预后因素。然而,对于结直肠癌(CRC)患者,其临床影响的研究有限且结果不一。
确定术前NLR(NLR-pre)、术后NLR(NLR-post)及其变化(NLR-delta)的最佳截断值,以最大化组间总生存期(OS)的差异。患者分为以下四组(NLR趋势):G1,术前和术后NLR均低;G2,术前NLR低且术后NLR高;G3,术前NLR高且术后NLR低;G4,术前和术后NLR均高。使用综合AUC(iAUC)比较所有指标的鉴别性能。
共纳入576例诊断为I-IV期CRC的患者。NLR-pre的截断点为2.33,NLR-post的截断点为2.06,NLR-delta的截断点为-1.08。单因素分析显示,使用NLR-pre、NLR-post、NLR-delta和NLR趋势进行亚组二分法均被确定为显著的预后因素。然而,在多因素分析中,只有NLR趋势仍然是独立的预后因素。NLR趋势的iAUC优于NLR-pre(自抽样iAUC平均差异=0.036;95%CI 0.013-0.073)、NLR-post(自抽样iAUC平均差异=0.045;95%CI 0.019-0.081)和NLR-delta(自抽样iAUC平均差异=0.061;95%CI 0.025-0.104)。
与CRC患者的NLR单次测量或简单变化相比,术前和术后NLR(NLR趋势)的风险分层和联合可改善预后鉴别。