Bischoff Jenny, Gu Wenyi, Schwarze-Zander Carolynne, Boesecke Christoph, Wasmuth Jan-Christian, van Bremen Kathrin, Dold Leona, Rockstroh Jürgen K, Trebicka Jonel
Department of Internal Medicine I, Venusberg Campus 1, University Hospital Bonn, 53127 Bonn Germany.
Department of Internal Medicine I, University Hospital Frankfurt, Germany.
EClinicalMedicine. 2021 Sep 5;40:101116. doi: 10.1016/j.eclinm.2021.101116. eCollection 2021 Oct.
De novo steatosis is the main criteria for non-alcoholic fatty liver disease (NAFLD), which is becoming a clinically relevant comorbidity in HIV-infected patients. This may be due to the HIV virus itself, as well as long-term toxicities deriving from antiretroviral therapy. Therefore, HIV infected patients require prevention and monitoring regarding NAFLD.
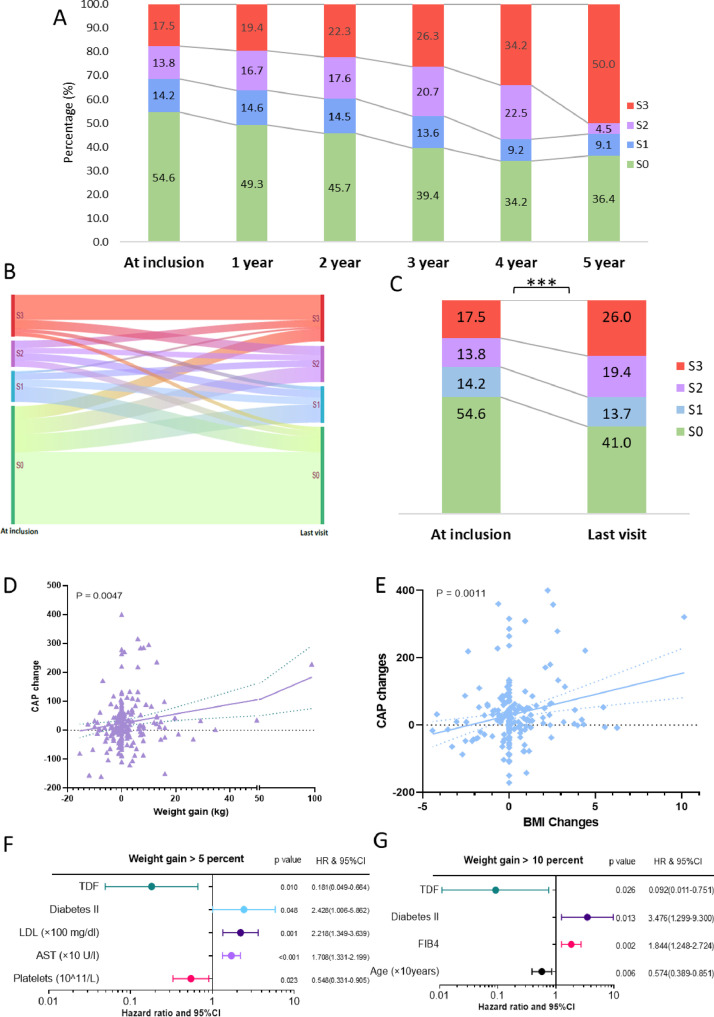
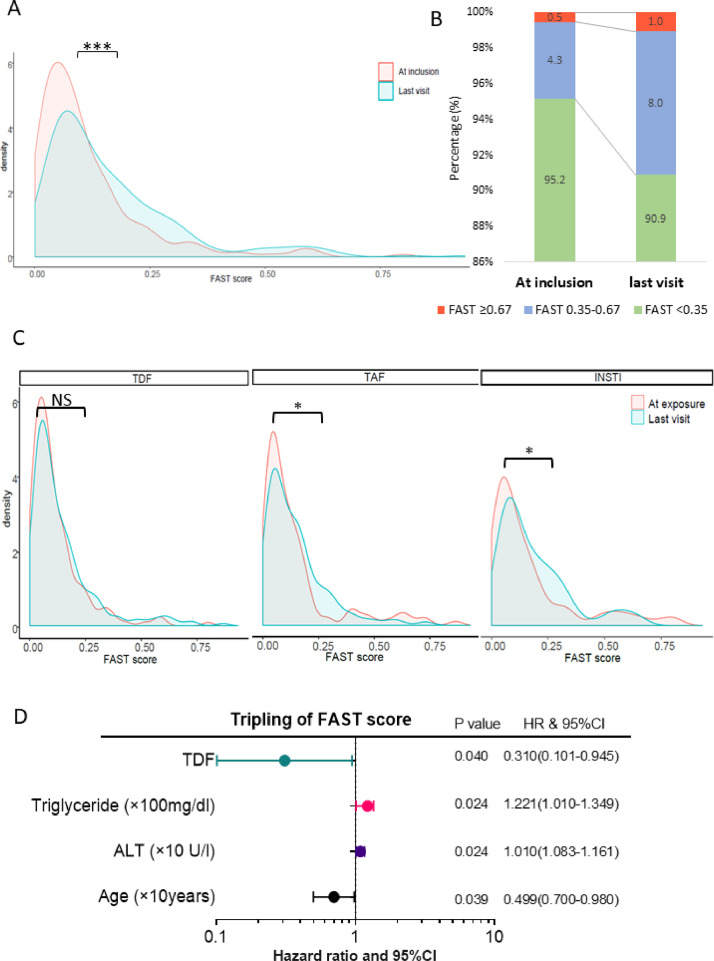
This study investigated the differential role of body mass index (BMI) and combination antiretroviral treatment (cART) drugs on NAFLD progression. This single center prospective longitudinal observational study enrolled HIV monoinfected individuals between August 2013 to December 2018 with yearly visits. Each visit included liver stiffness and steatosis [defined as controlled attenuation parameter (CAP)>237 dB/m] assessment by annually transient elastography using an M- or XL-probe of FibroScan, and calculation of the novel FibroScan-AST (FAST) score. Risk factors for denovo/progressed steatosis and tripling of FAST-score increase were investigated using Cox regression model with time-dependent covariates.
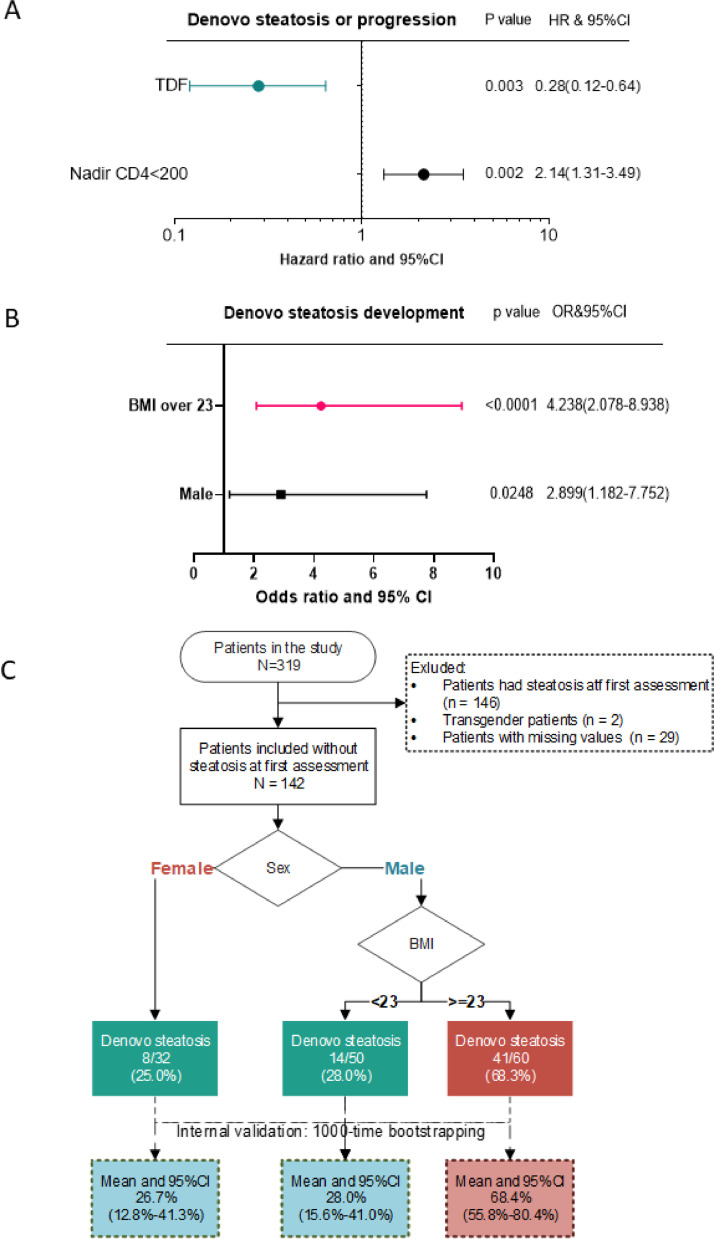
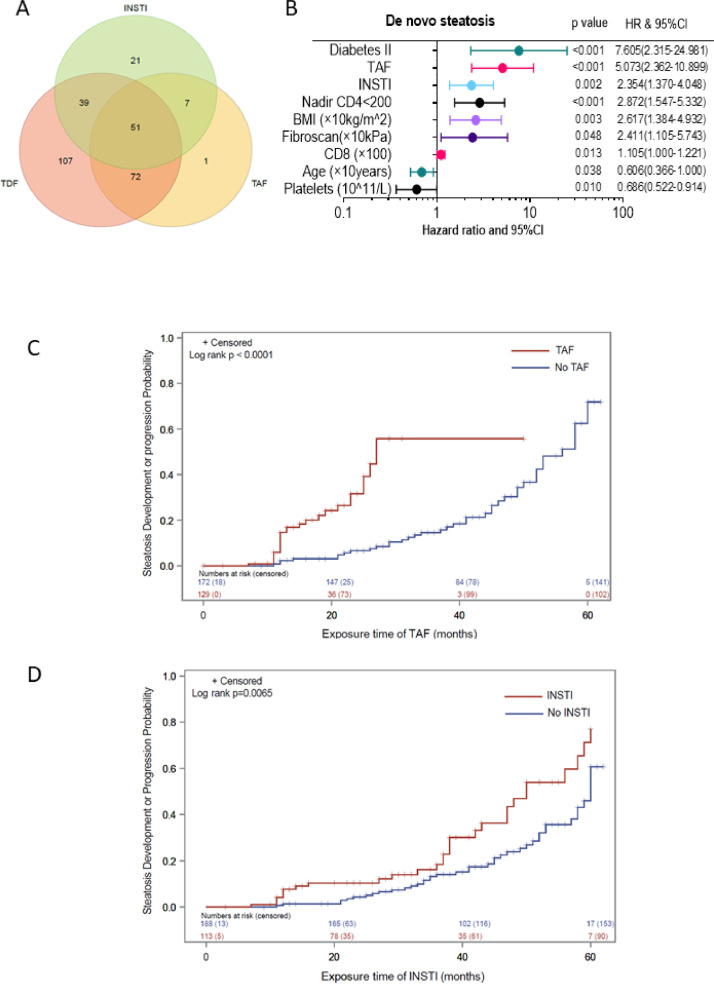
319 monoinfected HIV positive patients with at least two visits were included into the study, of which 301 patients had at least two valid CAP measurements. 51·5%(155) patients did not have steatosis at first assessment, of which 45%(69) developed steatosis during follow-up. A BMI>23 kg/m (OR: 4·238, 95% CI: 2·078-8·938; < 0·0001), tenofovir-alafenamid (TAF) (OR: 5·073, 95% CI: 2·362-10·899); < 0·0001) and integrase strand transfer inhibitors (INSTI) (OR: 2·354, 95% CI: 1·370-4·048; = 0·002), as well as type 2 diabetes mellitus (OR: 7·605, 95% CI: 2·315-24·981; < 0·0001) were independent predictors of de novo steatosis in multivariable analysis. Tenofovir disoproxilfumarate (TDF) was associated with a lower risk for weight gain and steatosis progression/onset using CAP value (HR: 0·28, 95% CI: 0·12-0·64; = 0·003) and FAST scores (HR: 0·31, 95% CI: 0·101-0·945; = 0·04).
Steatosis can develop despite non-obese BMI in patients with HIV monoinfection under cART, especially in male patients with BMI over 23 kg/m. While TAF and INSTI increase the risk of progression of steatosis, TDF was found to be independently associated with a lower risk of a clinically significant weight gain and thereby, might slow down development and progression of steatosis.
There was no additional funding received for this project. All funders mentioned in the 'declaration of interests' section had no influence on study design, data collection and analysis, decision to publish, or preparation of the manuscript.
新发脂肪变性是非酒精性脂肪性肝病(NAFLD)的主要标准,NAFLD在HIV感染患者中已成为一种具有临床相关性的合并症。这可能归因于HIV病毒本身以及抗逆转录病毒治疗产生的长期毒性。因此,HIV感染患者需要针对NAFLD进行预防和监测。
本研究调查了体重指数(BMI)和联合抗逆转录病毒治疗(cART)药物在NAFLD进展中的不同作用。这项单中心前瞻性纵向观察性研究纳入了2013年8月至2018年12月期间每年就诊的HIV单感染个体。每次就诊包括使用FibroScan的M型或XL型探头通过年度瞬时弹性成像评估肝脏硬度和脂肪变性[定义为控制衰减参数(CAP)>237 dB/m],并计算新的FibroScan-AST(FAST)评分。使用具有时间依赖性协变量的Cox回归模型研究新发/进展性脂肪变性和FAST评分增加三倍的危险因素。
319例至少就诊两次的单感染HIV阳性患者被纳入研究,其中301例患者有至少两次有效的CAP测量值。51.5%(155例)患者在首次评估时没有脂肪变性,其中45%(69例)在随访期间出现脂肪变性。在多变量分析中,BMI>23 kg/m(比值比:4.238,95%置信区间:2.078 - 8.938;P<0.0001)、替诺福韦艾拉酚胺(TAF)(比值比:5.073,95%置信区间:2.362 - 10.899;P<0.0001)、整合酶链转移抑制剂(INSTI)(比值比:2.354,95%置信区间:1.370 - 4.048;P = 0.002)以及2型糖尿病(比值比:7.605,95%置信区间:2.315 - 24.981;P<0.0001)是新发脂肪变性的独立预测因素。使用CAP值(风险比:0.28,95%置信区间:0.12 - 0.64;P = 0.003)和FAST评分(风险比:0.31,95%置信区间:0.101 - 0.945;P = 0.04)时,富马酸替诺福韦二吡呋酯(TDF)与体重增加和脂肪变性进展/发生风险较低相关。
接受cART的HIV单感染患者,即使BMI不高也可能发生脂肪变性,尤其是BMI超过23 kg/m的男性患者。虽然TAF和INSTI会增加脂肪变性进展的风险,但发现TDF与临床上显著体重增加的较低风险独立相关,因此可能减缓脂肪变性的发生和进展。
本项目未获得额外资助。“利益声明”部分提及的所有资助者对研究设计、数据收集和分析、出版决策或稿件准备均无影响。