Martino Marianna, Falcioni Paolo, Giancola Giulia, Ciarloni Alessandro, Salvio Gianmaria, Silvetti Francesca, Taccaliti Augusto, Arnaldi Giorgio
Division of Endocrinology and Metabolic Diseases, Department of Clinical and Molecular Sciences (DISCLIMO), Polytechnic University of Marche, Ancona, Italy.
Endocr Connect. 2021 Oct 15;10(10):1344-1351. doi: 10.1530/EC-21-0411.
Dysnatremia is common in hospitalized patients, often worsening the prognosis in pneumopathies and critical illnesses. Information on coronavirus disease-19 (COVID-19)-related hyponatremia is partially conflicting, whereas data on hypernatremia in this context are scarce. We assessed, in a cohort of COVID-19 inpatients: the prevalence of sodium alterations at admission and throughout their hospitalization; their association with inflammation/organ damage indexes; their short-term prognostic impact.
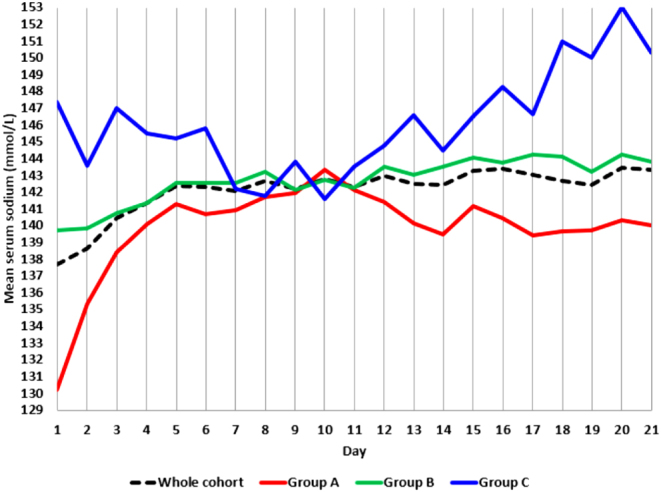
117 patients (81 males, 64 ± 13 years) hospitalized for COVID-19 between 1 March and 30 April 2020 were retrospectively followed-up for their first 21 days of stay by collecting all serum sodium measurements, basal CRP and serum lactate levels, maximum IL-6 and information on care setting, required ventilation, length of hospitalization, in-hospital death.
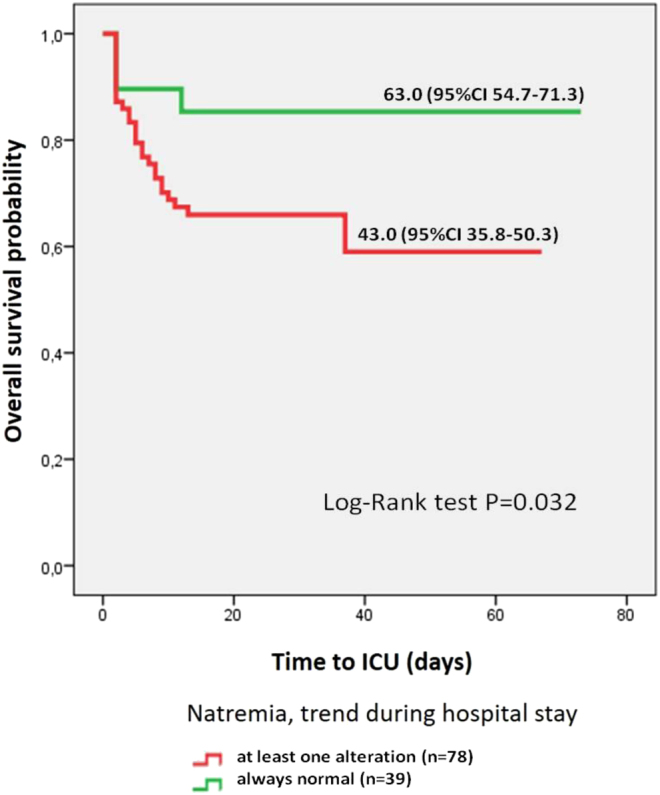
At admission, 26.5% patients had hyponatremia, and 6.8% had hypernatremia. During their hospitalization, 13.7% patients experienced both disorders ('mixed dysnatremia'). Lower sodium levels at admission were correlated with higher C reactive protein (CRP) (P = 0.039) and serum lactate levels (P = 0.019), but not interleukin-6 (IL-6). Hypernatremia and a wider sodium variability were associated with maximum required ventilation, need for ICU assistance and duration of the hospitalization. Mean estimated time to Intensive Care Unit (ICU) admission was 20 days shorter in patients exposed to sodium alterations at any time of their hospital course (log-rank test P = 0.032).
Sodium alterations frequently affect hospitalized COVID-19 patients. Hyponatremia could indicate pulmonary involvement, whereas hypernatremia is associated to prolonged hospitalization and the need for intensive care/mechanical ventilation, particularly when resulting from prior hyponatremia. Optimizing in-hospital sodium balance is crucial to improve patients' prognosis.
低钠血症在住院患者中很常见,常使肺病和危重病的预后恶化。关于冠状病毒病-19(COVID-19)相关低钠血症的信息存在部分矛盾,而关于这种情况下高钠血症的数据则很少。我们在一组COVID-19住院患者中评估了:入院时及整个住院期间钠改变的患病率;它们与炎症/器官损伤指标的关联;它们对短期预后的影响。
回顾性随访了2020年3月1日至4月30日因COVID-19住院的117例患者(81例男性,64±13岁),收集其住院前21天的所有血清钠测量值、基础CRP和血清乳酸水平、最高IL-6以及护理环境、所需通气、住院时间、院内死亡信息。
入院时,26.5%的患者有低钠血症,6.8%的患者有高钠血症。在住院期间,13.7%的患者出现了两种紊乱(“混合性钠紊乱”)。入院时较低的钠水平与较高的C反应蛋白(CRP)(P = 0.039)和血清乳酸水平(P = 0.019)相关,但与白细胞介素-6(IL-6)无关。高钠血症和更大的钠变异性与最大所需通气、ICU辅助需求和住院时间相关。在病程中任何时候出现钠改变的患者,其平均预计入住重症监护病房(ICU)的时间短20天(对数秩检验P = 0.032)。
钠改变经常影响住院的COVID-19患者。低钠血症可能表明肺部受累,而高钠血症与住院时间延长和重症监护/机械通气需求相关,特别是当由先前的低钠血症引起时。优化住院期间的钠平衡对于改善患者预后至关重要。