Endocrinology, Diabetes, and Metabolism, University Hospital Basel, Basel, Switzerland.
Endocrinology, Diabetes, and Metabolism, University Department of Medicine, Kantonsspital Aarau, Aarau, Switzerland.
J Clin Endocrinol Metab. 2020 Nov 1;105(11):3428-36. doi: 10.1210/clinem/dgaa547.
Hyponatremia has been associated with excess long-term morbidity and mortality. However, effects during hospitalization are poorly studied.
The objective of this work is to examine the association of hyponatremia with the risk of in-hospital mortality, 30-day readmission, and other short-term adverse events among medical inpatients.
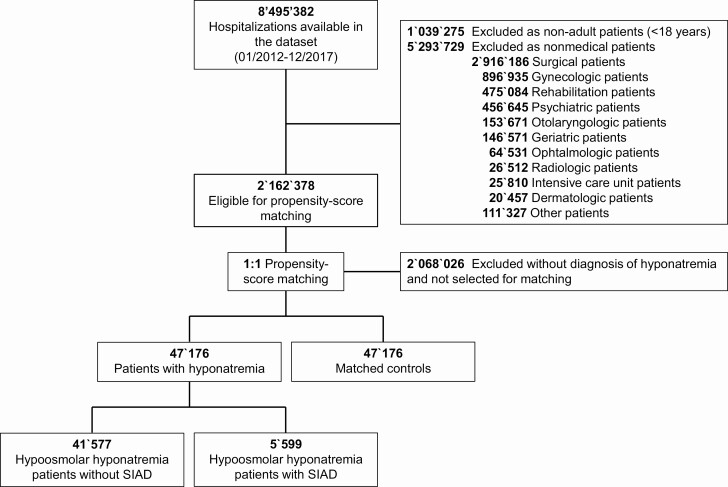
A population-based cohort study was conducted using a Swiss claims database of medical inpatients from January 2012 to December 2017.
Hyponatremic patients were 1:1 propensity-score matched with normonatremic medical inpatients.
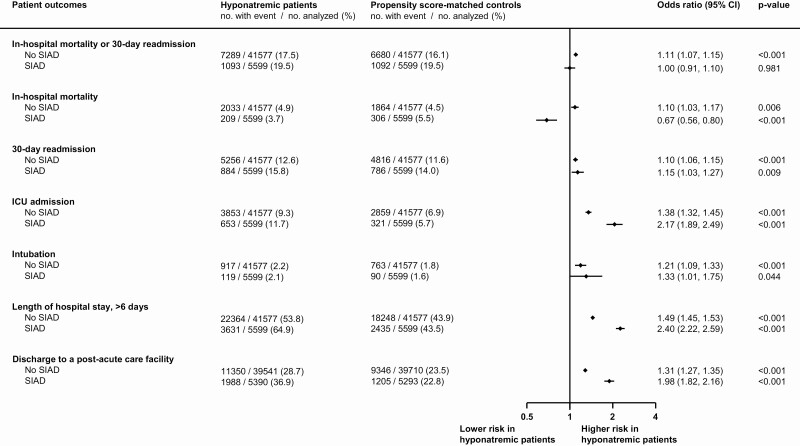
The primary outcome was a composite of all-cause in-hospital mortality and 30-day hospital readmission. Secondary outcomes were intensive care unit (ICU) admission, intubation rate, length-of-hospital stay (LOS), and patient disposition after discharge.
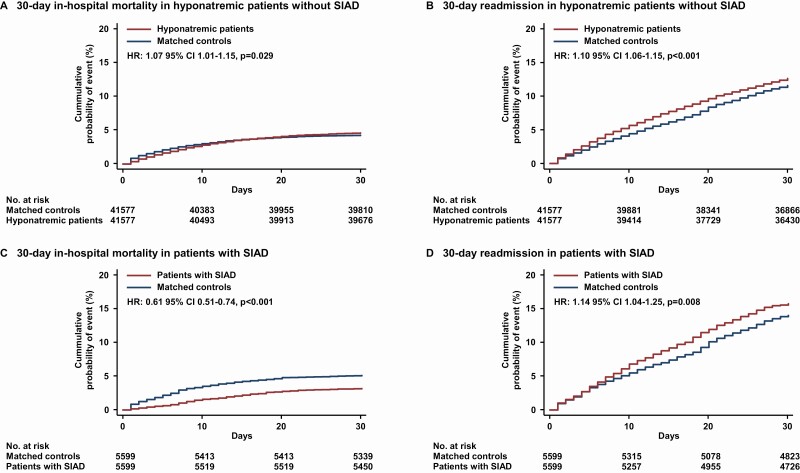
After matching, 94 352 patients were included in the cohort. Among 47 176 patients with hyponatremia, 8383 (17.8%) reached the primary outcome compared with 7994 (17.0%) in the matched control group (odds ratio [OR] 1.06 [95% CI, 1.02-1.10], P = .001). Hyponatremic patients were more likely to be admitted to the ICU (OR 1.43 [95% CI, 1.37-1.50], P < .001), faced a 56% increase in prolonged LOS (95% CI, 1.52-1.60, P < .001), and were admitted more often to a postacute care facility (OR 1.38 [95% CI 1.34-1.42, P < .001). Of note, patients with the syndrome of inappropriate antidiuresis (SIAD) had lower in-hospital mortality (OR 0.67 [95% CI, 0.56-0.80], P < .001) as compared with matched normonatremic controls.
In this study, hyponatremia was associated with increased risk of short-term adverse events, primarily driven by higher readmission rates, which was consistent among all outcomes except for decreased in-hospital mortality in SIAD patients.
低钠血症与长期过度发病率和死亡率有关。然而,住院期间的影响研究得还不够充分。
本研究旨在探讨低钠血症与住院期间的全因死亡率、30 天再入院率以及其他短期不良事件风险之间的相关性,研究对象为住院内科患者。
采用瑞士医疗住院患者索赔数据库,开展了一项基于人群的队列研究,研究对象为 2012 年 1 月至 2017 年 12 月的患者。
低钠血症患者与血压正常的内科住院患者进行 1:1 倾向评分匹配。
主要结局是全因住院期间死亡率和 30 天住院再入院率的复合结局。次要结局包括入住重症监护病房(ICU)、插管率、住院时间(LOS)和出院后的患者去向。
匹配后,共纳入 94352 例患者。在 47176 例低钠血症患者中,8383 例(17.8%)达到了主要结局,而在匹配对照组中,7994 例(17.0%)达到了主要结局(比值比[OR] 1.06[95%可信区间,1.02-1.10],P=0.001)。低钠血症患者更有可能被收入 ICU(OR 1.43[95%可信区间,1.37-1.50],P<0.001),LOS 延长的比例增加 56%(95%可信区间,1.52-1.60,P<0.001),更多地被收入康复护理机构(OR 1.38[95%可信区间,1.34-1.42],P<0.001)。值得注意的是,与匹配的血压正常对照组相比,抗利尿激素分泌不当综合征(SIAD)患者的住院期间死亡率较低(OR 0.67[95%可信区间,0.56-0.80],P<0.001)。
在本研究中,低钠血症与短期不良事件风险增加相关,这主要归因于再入院率升高,除 SIAD 患者的住院期间死亡率降低外,其他结局均如此。