Department of Neurology, Yale School of Medicine, New Haven, Connecticut, United States of America.
Equity Research and Innovation Center, Yale School of Medicine, New Haven, Connecticut, United States of America.
PLoS One. 2021 Sep 17;16(9):e0257608. doi: 10.1371/journal.pone.0257608. eCollection 2021.
Sequential Organ Failure Assessment (SOFA) score predicts probability of in-hospital mortality. Many crisis standards of care suggest the use of SOFA scores to allocate medical resources during the COVID-19 pandemic.
Are SOFA scores elevated among Non-Hispanic Black and Hispanic patients hospitalized with COVID-19, compared to Non-Hispanic White patients?
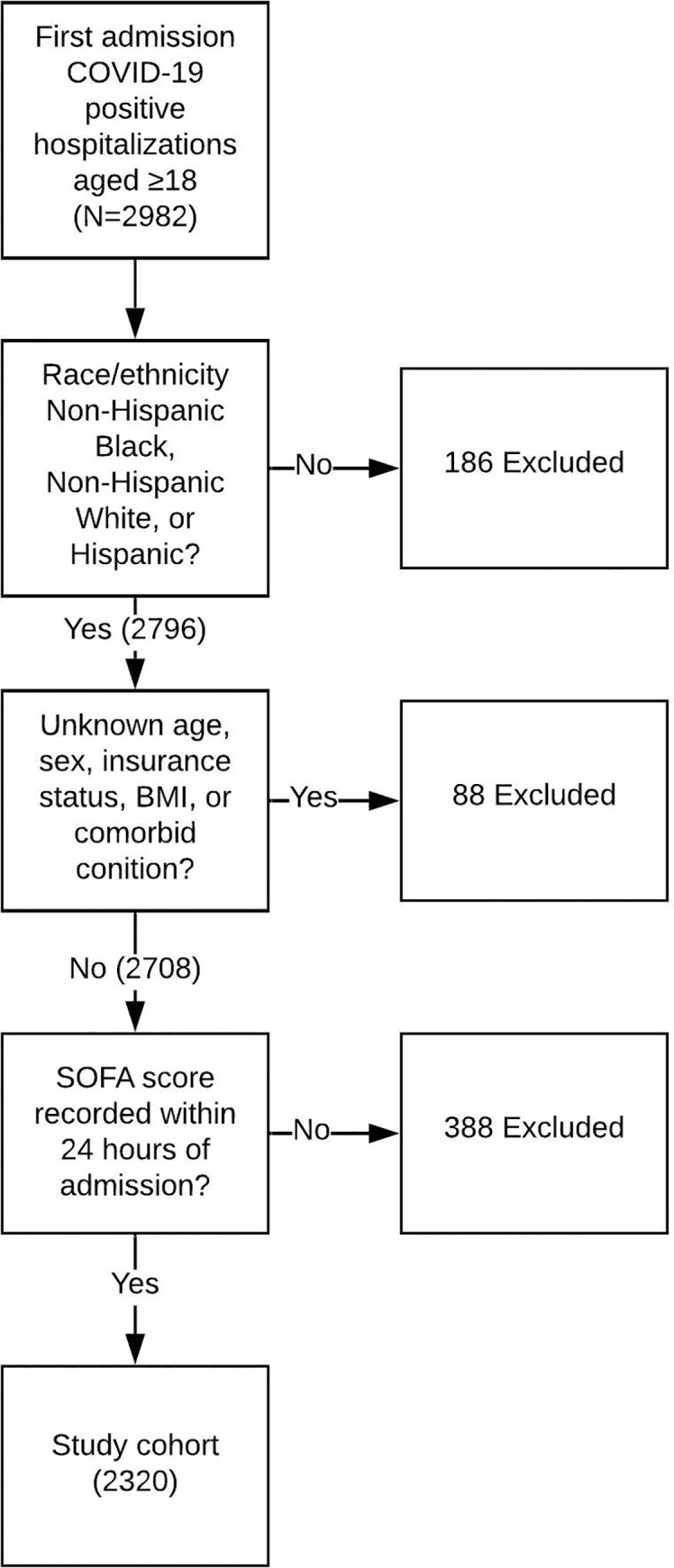
Retrospective cohort study conducted in Yale New Haven Health System, including 5 hospitals with total of 2681 beds. Study population drawn from consecutive patients aged ≥18 admitted with COVID-19 from March 29th to August 1st, 2020. Patients excluded from the analysis if not their first admission with COVID-19, if they did not have SOFA score recorded within 24 hours of admission, if race and ethnicity data were not Non-Hispanic Black, Non-Hispanic White, or Hispanic, or if they had other missing data. The primary outcome was SOFA score, with peak score within 24 hours of admission dichotomized as <6 or ≥6.
Of 2982 patients admitted with COVID-19, 2320 met inclusion criteria and were analyzed, of whom 1058 (45.6%) were Non-Hispanic White, 645 (27.8%) were Hispanic, and 617 (26.6%) were Non-Hispanic Black. Median age was 65.0 and 1226 (52.8%) were female. In univariate logistic screen and in full multivariate model, Non-Hispanic Black patients but not Hispanic patients had greater odds of an elevated SOFA score ≥6 when compared to Non-Hispanic White patients (OR 1.49, 95%CI 1.11-1.99).
Given current unequal patterns in social determinants of health, US crisis standards of care utilizing the SOFA score to allocate medical resources would be more likely to deny these resources to Non-Hispanic Black patients.
序贯器官衰竭评估 (SOFA) 评分可预测住院患者死亡率。许多危重病护理标准建议在 COVID-19 大流行期间使用 SOFA 评分来分配医疗资源。
与非西班牙裔白人患者相比,因 COVID-19 住院的非西班牙裔黑人和西班牙裔患者的 SOFA 评分是否升高?
这是在耶鲁纽黑文卫生系统进行的回顾性队列研究,包括 5 家拥有 2681 张床位的医院。研究人群来自 2020 年 3 月 29 日至 8 月 1 日连续因 COVID-19 入院且年龄≥18 岁的患者。如果患者不是首次因 COVID-19 入院、入院 24 小时内未记录 SOFA 评分、种族和族裔数据不是非西班牙裔黑人、非西班牙裔白人或西班牙裔,或者如果患者存在其他缺失数据,则将其从分析中排除。主要结局是 SOFA 评分,入院 24 小时内的最高评分分为<6 或≥6。
在 2982 名因 COVID-19 入院的患者中,有 2320 名符合纳入标准并进行了分析,其中 1058 名(45.6%)为非西班牙裔白人,645 名(27.8%)为西班牙裔,617 名(26.6%)为非西班牙裔黑人。中位年龄为 65.0 岁,1226 名(52.8%)为女性。在单变量逻辑筛选和全多变量模型中,与非西班牙裔白人患者相比,非西班牙裔黑人患者而非西班牙裔黑人患者的 SOFA 评分升高(OR 1.49,95%CI 1.11-1.99)。
鉴于当前社会决定因素在健康方面的不平等模式,美国利用 SOFA 评分来分配医疗资源的危重病护理标准更有可能拒绝向非西班牙裔黑人患者提供这些资源。