Division of Pulmonary, Critical Care, and Sleep Medicine.
Division of Critical Care Medicine, Albert Einstein College of Medicine, Bronx, New York; and.
Ann Am Thorac Soc. 2022 May;19(5):790-798. doi: 10.1513/AnnalsATS.202106-680OC.
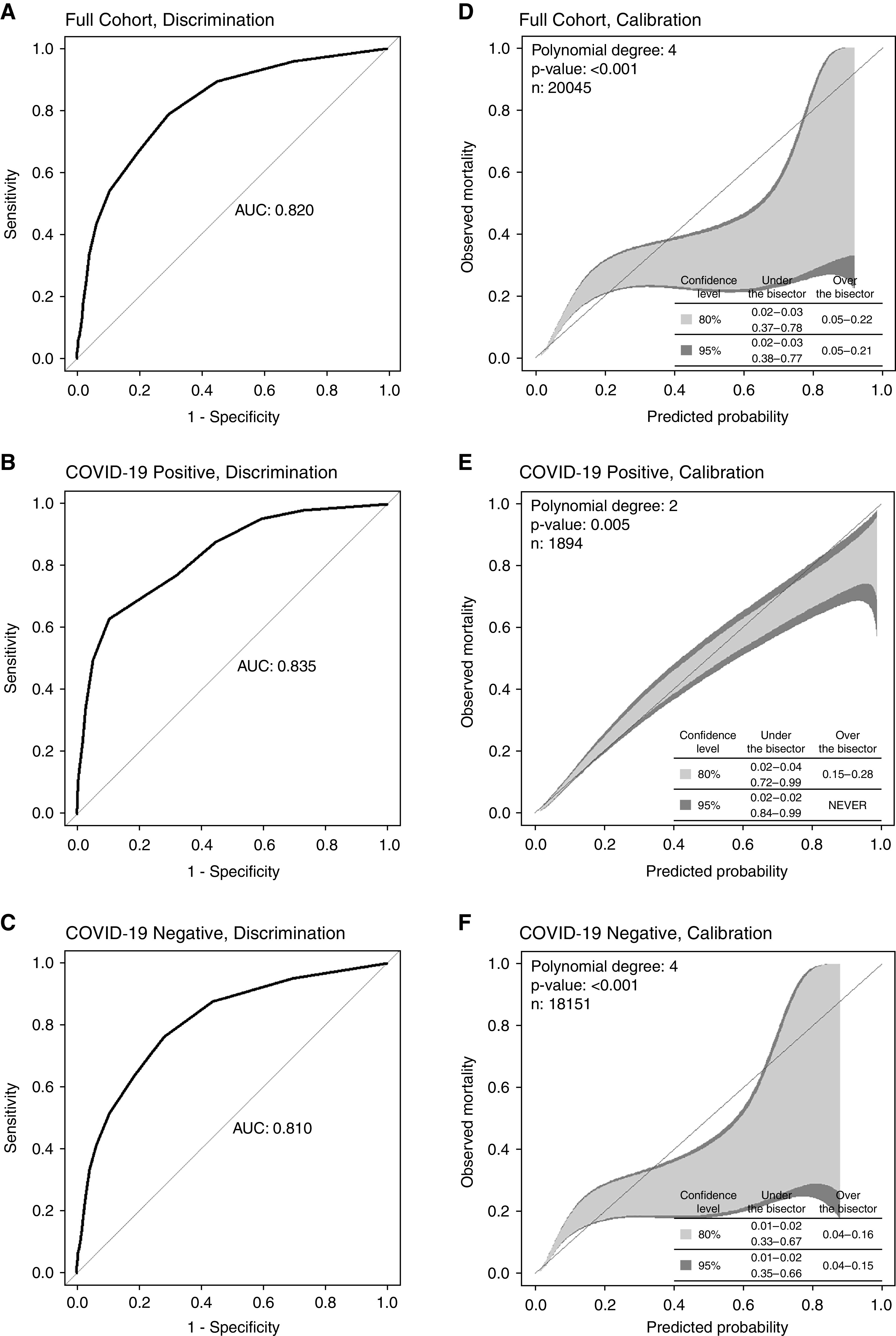
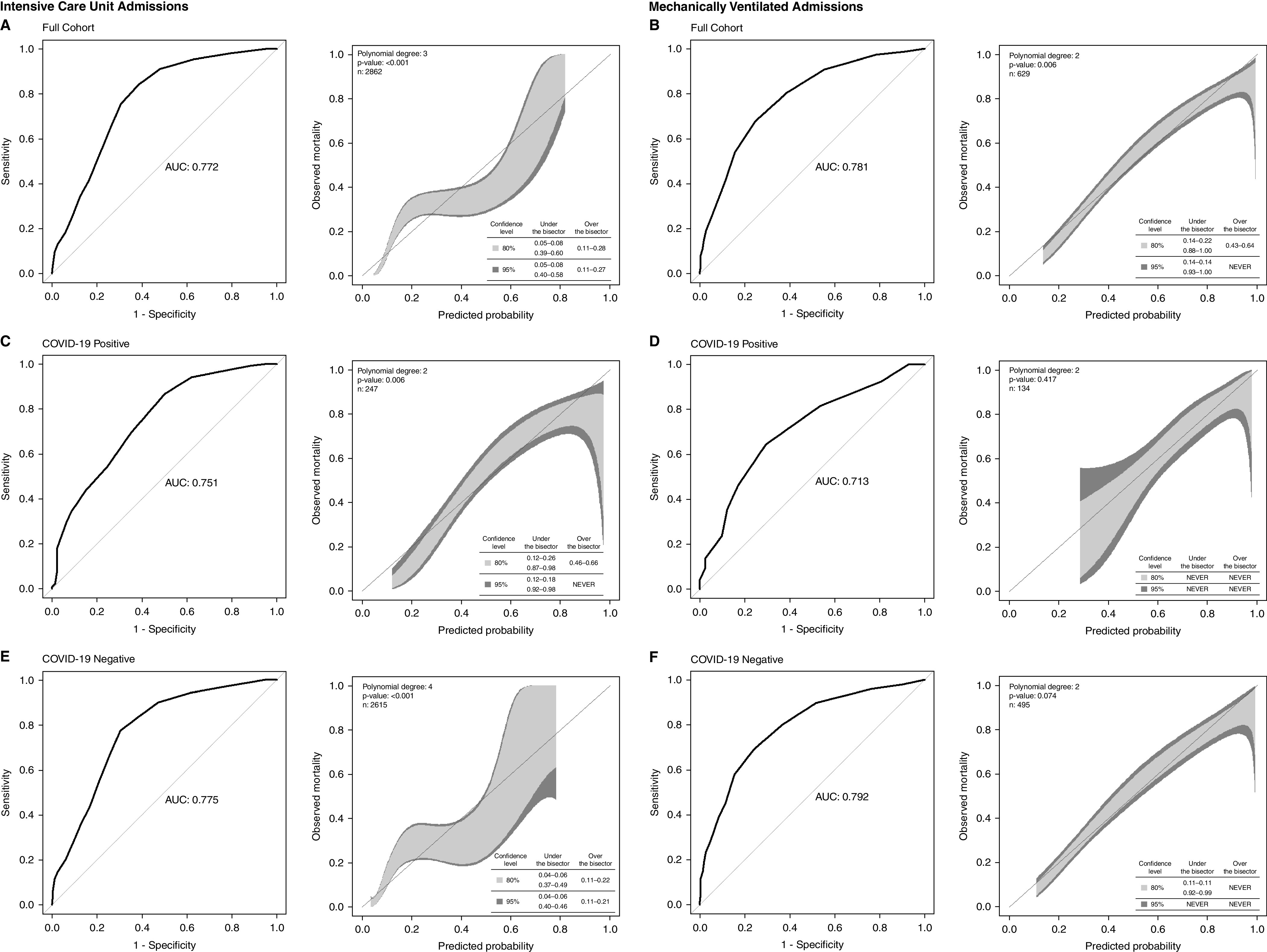
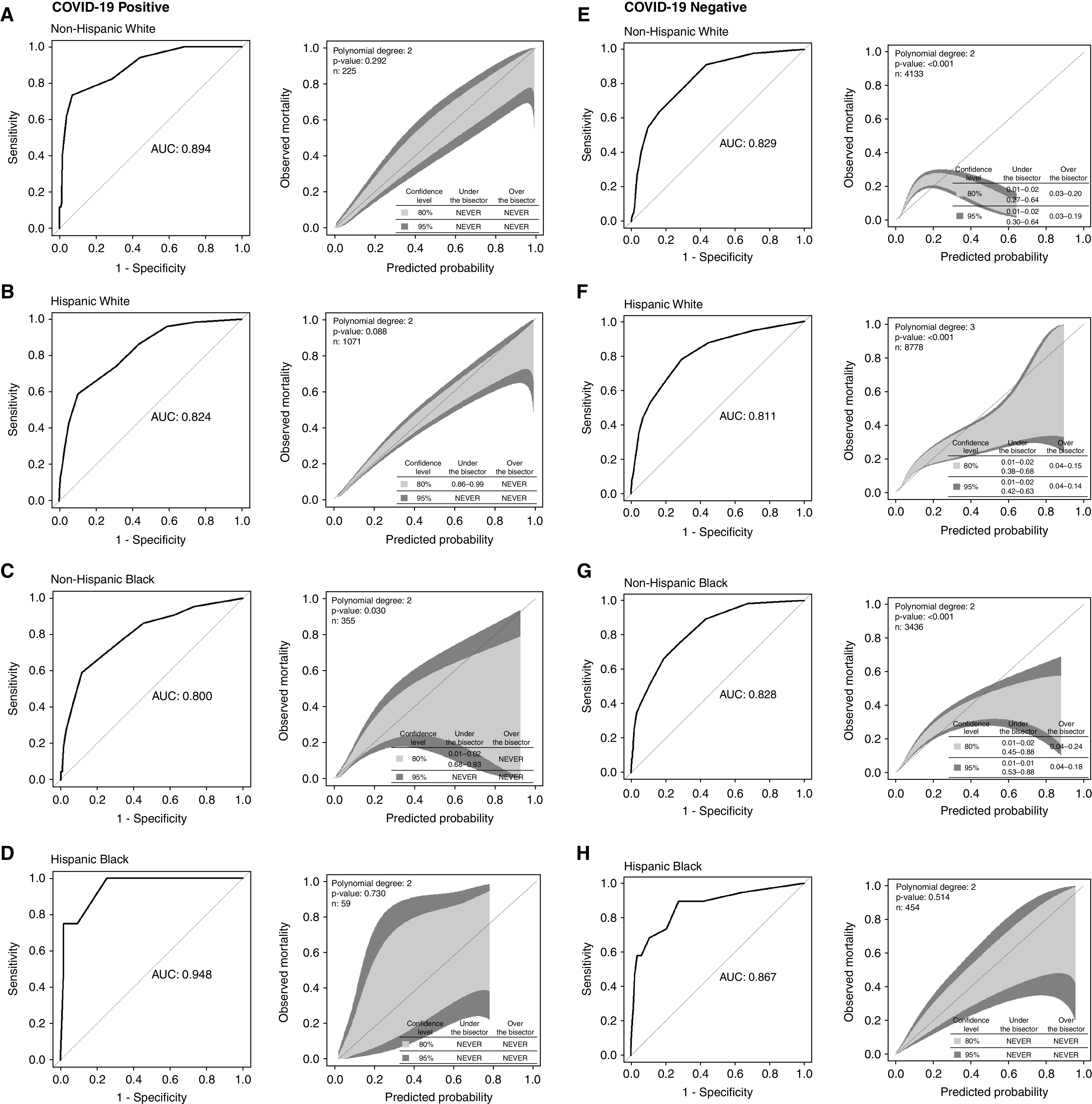
Sequential organ failure assessment (SOFA) scores are commonly used in crisis standards of care policies to assist in resource allocation. The relative predictive value of SOFA by coronavirus disease (COVID-19) infection status and among racial and ethnic subgroups within patients infected with COVID-19 is unknown. To evaluate the accuracy and calibration of SOFA in predicting hospital mortality by COVID-19 infection status and across racial and ethnic subgroups. We performed a retrospective cohort study of adult admissions to the University of Miami Hospital and Clinics inpatient wards (July 1, 2020-April 1, 2021). We primarily considered maximum SOFA within 48 hours of hospitalization. We assessed accuracy using the area under the receiver operating characteristic curve (AUROC) and created calibration belts. Considered subgroups were defined by COVID-19 infection status (by severe acute respiratory syndrome coronavirus 2 polymerase chain reaction testing) and prevalent racial and ethnic minorities. Comparisons across subgroups were made with DeLong testing for discriminative accuracy and visualization of calibration belts. Our primary cohort consisted of 20,045 hospitalizations, of which 1,894 (9.5%) were COVID-19 positive. SOFA was similarly accurate for COVID-19-positive (AUROC, 0.835) and COVID-19-negative (AUROC, 0.810; = 0.15) admissions but was slightly better calibrated in patients who were positive for COVID-19. For those with critical illness, maximum SOFA score accuracy at critical illness onset also did not differ by COVID-19 status (AUROC, COVID-19 positive vs. negative: intensive care unit admissions, 0.751 vs. 0.775; = 0.46; mechanically ventilated, 0.713 vs. 0.792, = 0.13), and calibration was again better for patients positive for COVID-19. Among patients with COVID-19, SOFA accuracy was similar between the non-Hispanic White population (AUROC, 0.894) and racial and ethnic minorities (Hispanic White population: AUROC, 0.824 [ vs. non-Hispanic White = 0.05]; non-Hispanic Black population: AUROC, 0.800 [ = 0.12]; Hispanic Black population: AUROC, 0.948 [ = 0.31]). This similar accuracy was also found for those without COVID-19 (non-Hispanic White population: AUROC, 0.829; Hispanic White population: AUROC, 0.811 [ = 0.37]; Hispanic Black population: AUROC, 0.828 [ = 0.97]; non-Hispanic Black population: AUROC, 0.867 [ = 0.46]). SOFA was well calibrated for all racial and ethnic groups with COVID-19 but estimated mortality more variably and performed less well across races and ethnicities without COVID-19. SOFA accuracy does not differ by COVID-19 status and is similar among racial and ethnic groups both with and without COVID-19. Calibration is better for COVID-19-infected patients and, among those without COVID-19, varies by race and ethnicity.
序贯器官衰竭评估 (SOFA) 评分常用于危机标准护理政策,以协助资源分配。冠状病毒病 (COVID-19) 感染状态和 COVID-19 感染患者中种族和民族亚组的 SOFA 相对预测值尚不清楚。本研究旨在评估 SOFA 在预测 COVID-19 感染状态和不同种族和民族亚组患者住院死亡率方面的准确性和校准情况。我们对迈阿密大学医院和诊所住院病房(2020 年 7 月 1 日至 2021 年 4 月 1 日)的成年患者进行了回顾性队列研究。我们主要考虑住院后 48 小时内的最大 SOFA。我们使用接受者操作特征曲线下面积 (AUROC) 评估准确性,并创建校准带。考虑的亚组通过严重急性呼吸综合征冠状病毒 2 聚合酶链反应检测来定义 COVID-19 感染状态和常见的少数族裔。使用 DeLong 检验比较亚组间的差异,以评估区分准确性和校准带的可视化。我们的主要队列包括 20,045 例住院患者,其中 1,894 例(9.5%)COVID-19 检测呈阳性。COVID-19 阳性(AUROC,0.835)和 COVID-19 阴性(AUROC,0.810; = 0.15)患者的 SOFA 准确性相似,但 COVID-19 感染患者的校准情况稍好。对于患有危重病的患者,发病时最大 SOFA 评分的准确性也不因 COVID-19 状态而异(COVID-19 阳性与阴性:重症监护病房入院,0.751 与 0.775; = 0.46;机械通气,0.713 与 0.792, = 0.13),并且 COVID-19 感染患者的校准情况再次更好。在 COVID-19 患者中,SOFA 准确性在非西班牙裔白人人群(AUROC,0.894)和少数族裔之间相似(西班牙裔白人人群:AUROC,0.824 [与非西班牙裔白人相比 = 0.05];非西班牙裔黑人人群:AUROC,0.800 [ = 0.12];西班牙裔黑人人群:AUROC,0.948 [ = 0.31])。对于没有 COVID-19 的患者,也发现了类似的准确性(非西班牙裔白人人群:AUROC,0.829;西班牙裔白人人群:AUROC,0.811 [ = 0.37];西班牙裔黑人人群:AUROC,0.828 [ = 0.97];非西班牙裔黑人人群:AUROC,0.867 [ = 0.46])。SOFA 在 COVID-19 患者中具有良好的校准,但在没有 COVID-19 的患者中,估计死亡率的变化更大,并且在不同种族和民族中表现不佳。SOFA 准确性不因 COVID-19 状态而异,在 COVID-19 患者和非 COVID-19 患者中,种族和民族之间的准确性相似。在 COVID-19 感染患者中,校准情况更好,而在非 COVID-19 患者中,校准情况因种族和民族而异。