Huang Liebin, Feng Bao, Li Yueyue, Liu Yu, Chen Yehang, Chen Qinxian, Li Changlin, Huang Wensi, Xue Huimin, Li Xuehua, Zhou Tao, Li Ronggang, Long Wansheng, Feng Shi-Ting
Department of Radiology, Jiangmen Central Hospital, Jiangmen, China.
School of Electronic Information and Automation, Guilin University of Aerospace Technology, Guilin, China.
Front Oncol. 2021 Sep 2;11:638362. doi: 10.3389/fonc.2021.638362. eCollection 2021.
Accurate prediction of postoperative recurrence risk of gastric cancer (GC) is critical for individualized precision therapy. We aimed to investigate whether a computed tomography (CT)-based radiomics nomogram can be used as a tool for predicting the local recurrence (LR) of GC after radical resection.
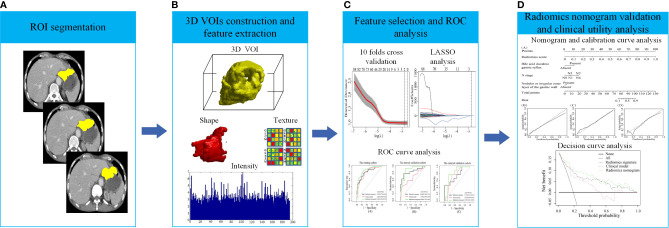
342 patients (194 in the training cohort, 78 in the internal validation cohort, and 70 in the external validation cohort) with pathologically proven GC from two centers were included. Radiomics features were extracted from the preoperative CT imaging. The clinical model, radiomics signature, and radiomics nomogram, which incorporated the radiomics signature and independent clinical risk factors, were developed and verified. Furthermore, the performance of these three models was assessed by using the area under the curve (AUC) of receiver operating characteristic (ROC) curve analysis and decision curve analysis (DCA).
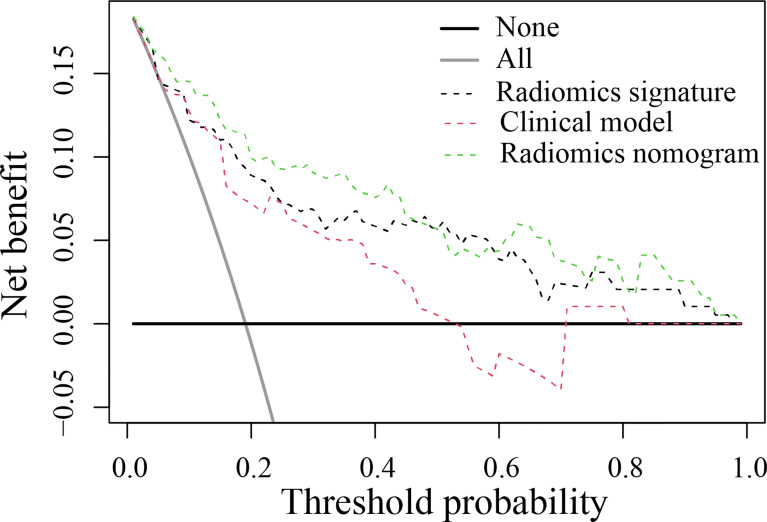
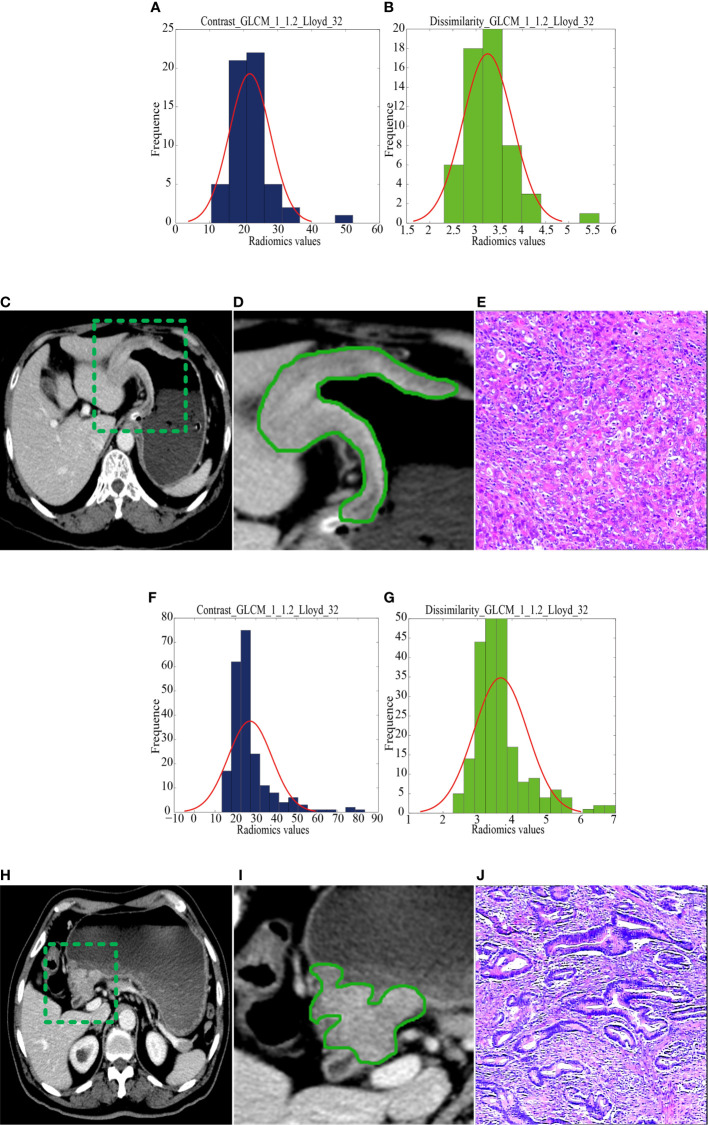
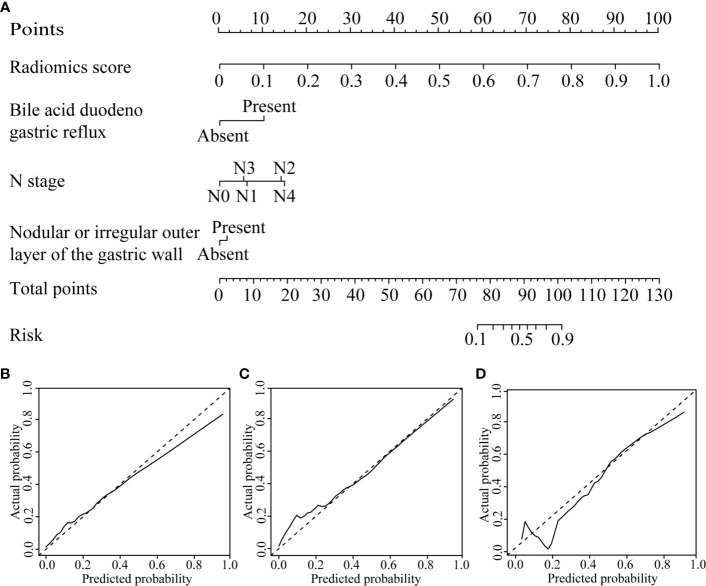
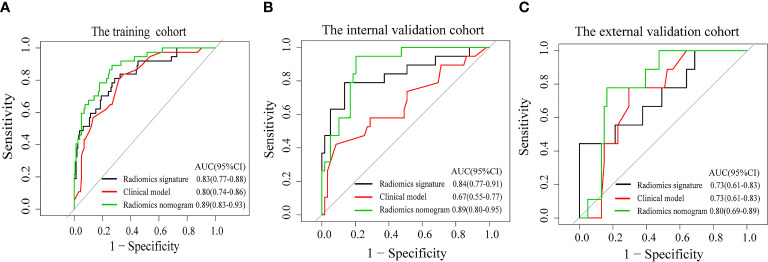
The radiomics signature, which was comprised of two selected radiomics features, namely, contrast_GLCM and dissimilarity_GLCM, showed better performance than the clinical model in predicting the LR of GC, with AUC values of 0.83 in the training cohort, 0.84 in the internal validation cohort, and 0.73 in the external cohort, respectively. By integrating the independent clinical risk factors (N stage, bile acid duodenogastric reflux and nodular or irregular outer layer of the gastric wall) into the radiomics signature, the radiomics nomogram achieved the highest accuracy in predicting LR, with AUC values of 0.89, 0.89 and 0.80 in the three cohorts, respectively. DCA in the validation cohort showed that radiomics nomogram added more net benefit than the clinical model within the range of 0.01-0.98.
The CT-based radiomics nomogram has the potential to predict the LR of GC after radical resection.
准确预测胃癌(GC)术后复发风险对个体化精准治疗至关重要。我们旨在研究基于计算机断层扫描(CT)的影像组学列线图是否可作为预测根治性切除术后GC局部复发(LR)的工具。
纳入来自两个中心的342例经病理证实的GC患者(训练队列194例,内部验证队列78例,外部验证队列70例)。从术前CT影像中提取影像组学特征。构建并验证了临床模型、影像组学特征以及结合影像组学特征和独立临床危险因素的影像组学列线图。此外,通过受试者操作特征(ROC)曲线分析的曲线下面积(AUC)和决策曲线分析(DCA)评估这三种模型的性能。
由两个选定的影像组学特征,即对比度_GLCM和差异度_GLCM组成的影像组学特征在预测GC的LR方面表现优于临床模型,训练队列、内部验证队列和外部队列的AUC值分别为0.83、0.84和0.73。通过将独立临床危险因素(N分期、胆汁酸十二指肠胃反流和胃壁结节状或不规则外层)纳入影像组学特征,影像组学列线图在预测LR方面达到了最高准确率,三个队列的AUC值分别为0.89、0.89和0.80。验证队列中的DCA显示,在0.01 - 0.98范围内,影像组学列线图比临床模型增加了更多的净效益。
基于CT的影像组学列线图有潜力预测根治性切除术后GC的LR。