Heart Failure and Structural Cardiology Division, First Affiliated Hospital of Dalian Medical University, Dalian, China.
Kent and Medway Medical School, Canterbury, UK.
ESC Heart Fail. 2021 Dec;8(6):5383-5391. doi: 10.1002/ehf2.13630. Epub 2021 Sep 27.
There is an emerging interest in elucidating the natural history and prognosis for patients with heart failure with reduced ejection fraction (HFrEF) in whom left ventricular ejection fraction (LVEF) subsequently improves. The characteristics and outcomes were compared between heart failure with recovered ejection fraction (HFrecEF) and persistent HFrEF.
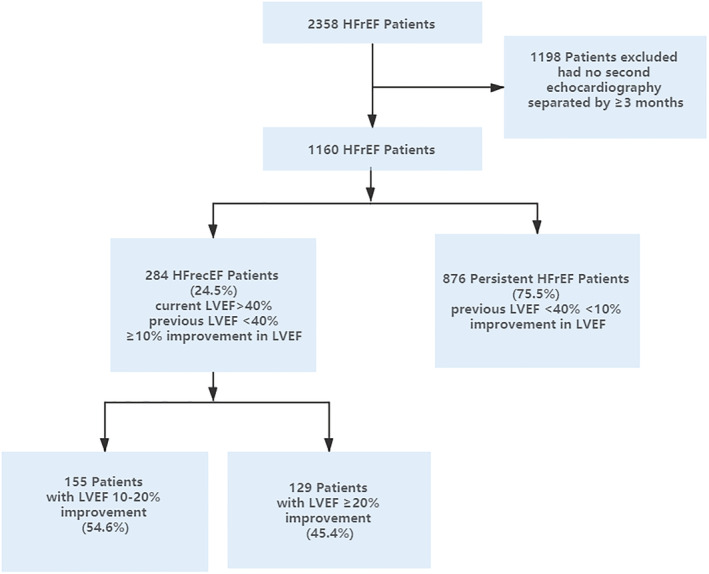
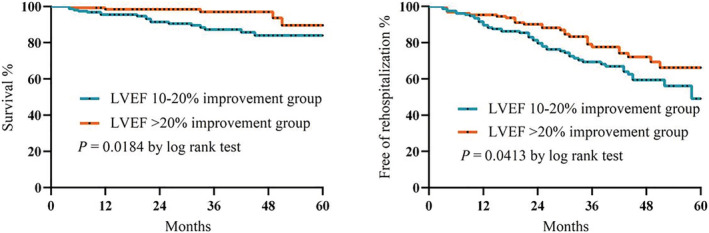
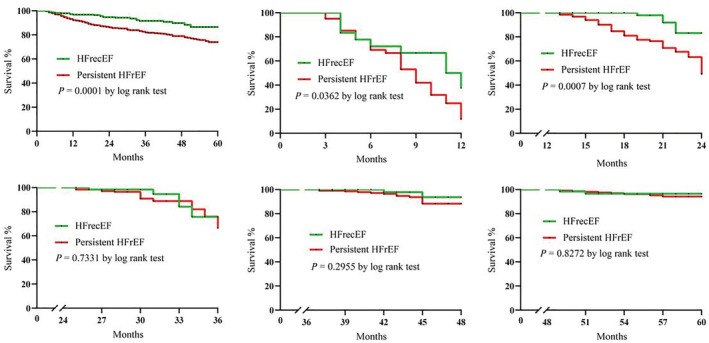
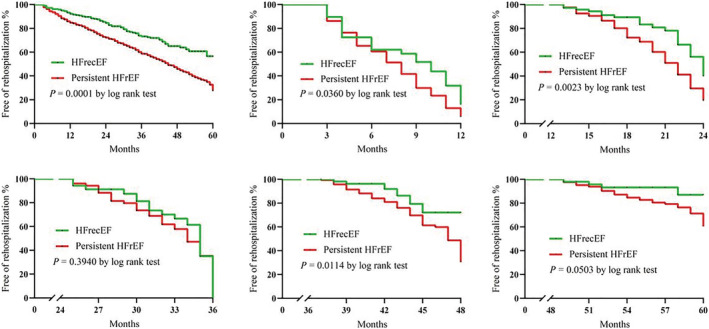
This is a retrospective study of adults who underwent at least two echocardiograms 3 months apart between 1 November 2015 and 31 October 2019 with an initial diagnosis of HFrEF. The subjects were divided into HFrecEF group (second LVEF > 40%, ≥10% absolute improvement in LVEF) and persistent HFrEF group (<10% absolute improvement in LVEF) according to the second LVEF. To further study the characteristics of HFrecEF patients, the cohort was further divided into LVEF improvement of 10-20% and >20% subgroups. The primary outcomes were all-cause mortality and rehospitalization. A total of 1160 HFrEF patients were included [70.2% male, mean (standard deviation) age: 62 ± 13 years]. On the second echocardiogram, 284 patients (24.5%) showed HFrecEF and 876 patients (75.5%) showed persistent HFrEF. All-cause mortality was identified in 23 (8.10%) HFrecEF and 165 (18.84%) persistent HFrEF, whilst 76 (26.76%) and 426 (48.63%) showed rehospitalizations, respectively. Survival analysis showed that the persistent HFrEF subgroup experienced a significantly higher mortality at 12 and 24 months and a higher hospitalization at 12, 24, 48, and more than 48 months following discharge. Multivariate Cox regression showed that persistent HFrEF had a higher risk of all-cause mortality [hazard ratio (HR) 2.30, 95% confidence interval (CI) 1.49-3.56, P = 0.000] and rehospitalization (HR 1.85, 95% CI 1.45-2.36, P = 0.000) than the HFrecEF group. Subgroup analysis showed that the LVEF ≥ 20% improvement subgroup had lower rates of adverse outcomes compared with those with less improvement of 10-20%.
Heart failure with recovered ejection fraction is a distinct HF phenotype with better clinical outcomes compared with those with persistent HFrEF. HFrecEF patients have a relatively better short-term mortality at 24 months but not thereafter.
人们对射血分数降低的心力衰竭(HFrEF)患者中左心室射血分数(LVEF)随后改善的自然史和预后越来越感兴趣。本研究比较了恢复射血分数的心力衰竭(HFrecEF)和持续性 HFrEF 患者的特征和结局。
这是一项回顾性研究,纳入了 2015 年 11 月 1 日至 2019 年 10 月 31 日期间至少两次相隔 3 个月的超声心动图检查且初始诊断为 HFrEF 的成年人。根据第二次 LVEF 将患者分为 HFrecEF 组(第二次 LVEF>40%,LVEF 绝对改善≥10%)和持续性 HFrEF 组(LVEF 绝对改善<10%)。为了进一步研究 HFrecEF 患者的特征,将该队列进一步分为 LVEF 改善 10-20%和>20%亚组。主要结局为全因死亡率和再住院率。共纳入 1160 例 HFrEF 患者[70.2%为男性,平均(标准差)年龄:62±13 岁]。在第二次超声心动图检查时,284 例(24.5%)患者出现 HFrecEF,876 例(75.5%)患者出现持续性 HFrEF。HFrecEF 中有 23 例(8.10%)和持续性 HFrEF 中有 165 例(18.84%)发生全因死亡,HFrecEF 中有 76 例(26.76%)和持续性 HFrEF 中有 426 例(48.63%)发生再住院。生存分析显示,持续性 HFrEF 亚组在 12 个月和 24 个月时的死亡率显著更高,在出院后 12、24、48 和超过 48 个月时的再住院率也更高。多变量 Cox 回归显示,持续性 HFrEF 发生全因死亡[风险比(HR)2.30,95%置信区间(CI)1.49-3.56,P=0.000]和再住院(HR 1.85,95% CI 1.45-2.36,P=0.000)的风险均高于 HFrecEF 组。亚组分析显示,LVEF 改善≥20%的亚组与改善 10-20%的亚组相比,不良结局发生率较低。
与持续性 HFrEF 相比,恢复射血分数的心力衰竭是一种明显不同的心力衰竭表型,具有更好的临床结局。HFrecEF 患者在 24 个月时的短期死亡率相对较低,但此后并非如此。