Nephrology Department, Fundeni Clinical Institute, 022328 Bucharest, Romania.
Nephrology Department, "Carol Davila" University of Medicine and Pharmacy, 050471 Bucharest, Romania.
Medicina (Kaunas). 2021 Aug 31;57(9):912. doi: 10.3390/medicina57090912.
Kidney involvement is a frequent complication of systemic lupus erythematosus (SLE) and kidney biopsy is essential in differentiating lupus nephritis (LN) from thrombotic microangiopathy (TMA) secondary to antiphospholipid autoantibodies (aPL). Association between antiphospholipid syndrome (APS) and acquired hemophilia due to inhibitors was very rarely described in SLE patients.
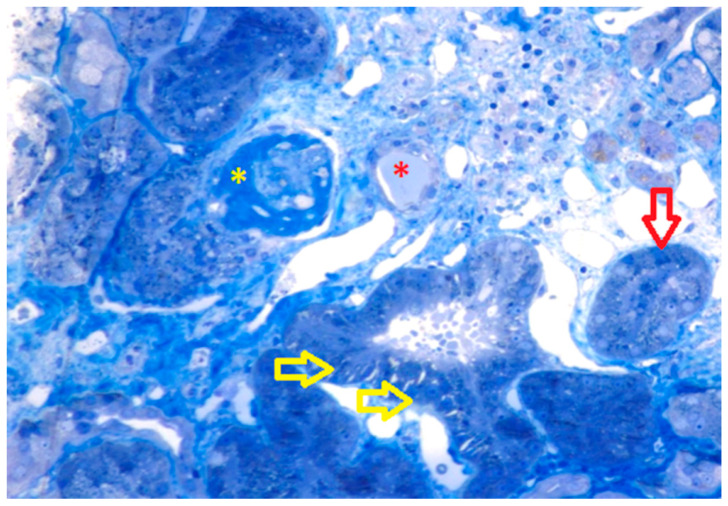
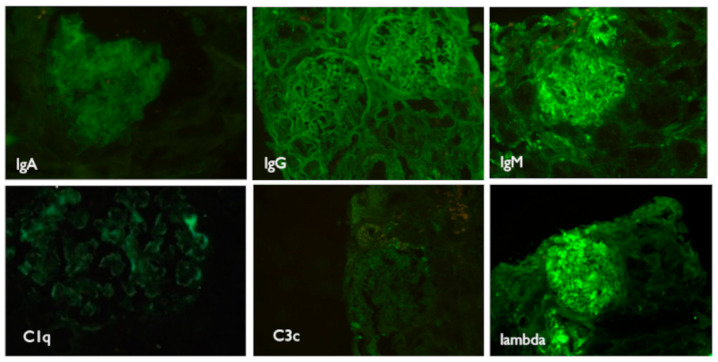
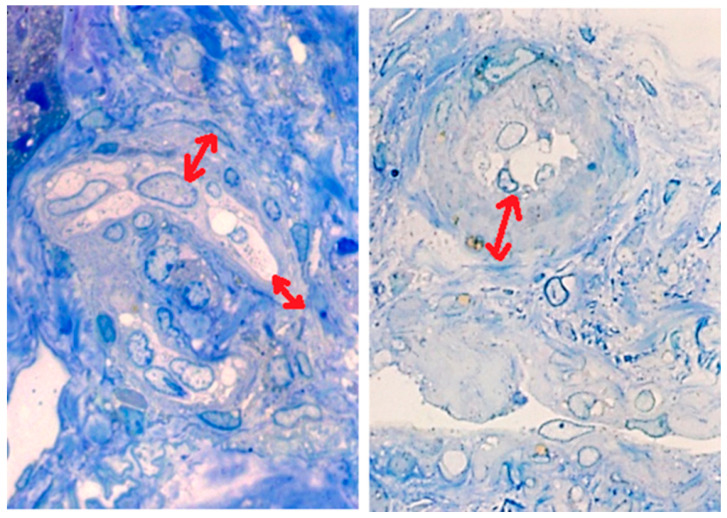
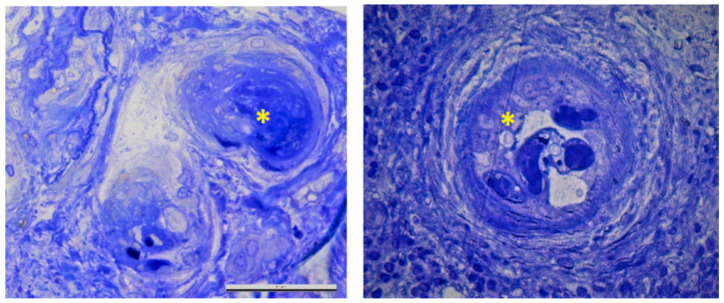
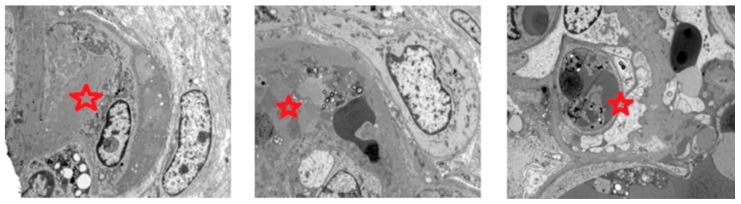
We present the case of a 61-year-old male diagnosed with SLE who acquired deficiency of clotting factor VIII due to circulating inhibitors, admitted for acute kidney injury (AKI), microangiopathic hemolytic anemia, thrombocytopenia, and diplopia. Kidney biopsy showed TMA due to APS, but no signs of LN. Head computed tomography identified low dense areas in the white matter, suggesting small blood vessels' involvement. A diagnosis of probable catastrophic antiphospholipid syndrome (CAPS) was established and treatment with low molecular weight heparin, intravenous methylprednisolone, plasmapheresis, and rituximab was initiated, followed by resolution of AKI, diplopia, and TMA with complete depletion of CD19+B-lymphocytes (CD19+B-Ly) after one month. We further review the current knowledge regarding pathogenesis and management of CAPS in SLE patients.
Targeted therapy was possible after kidney biopsy, improving renal and general prognosis. CD19+B-Ly repopulation preceded biological relapse, so monitoring of CD19+B-Ly may serve as a tool to predict relapses and guide rituximab therapy.
肾脏受累是系统性红斑狼疮(SLE)的常见并发症,肾活检对于区分狼疮性肾炎(LN)与抗磷脂自身抗体(aPL)继发的血栓性微血管病(TMA)至关重要。抗磷脂综合征(APS)与因抑制剂导致的获得性血友病在 SLE 患者中非常罕见。
我们报告了一例 61 岁男性 SLE 患者,因循环抑制剂导致凝血因子 VIII 缺乏,因急性肾损伤(AKI)、微血管性溶血性贫血、血小板减少和复视而入院。肾活检显示由 APS 引起的 TMA,但无 LN 迹象。头颅计算机断层扫描发现脑白质有低密区,提示小血管受累。诊断为可能的灾难性抗磷脂综合征(CAPS),并开始使用低分子肝素、静脉注射甲基强的松龙、血浆置换和利妥昔单抗治疗,一个月后 AKI、复视和 TMA 完全缓解,CD19+B 淋巴细胞(CD19+B-Ly)完全耗竭。我们进一步复习了关于 SLE 患者中 CAPS 的发病机制和治疗的现有知识。
肾活检后可以进行靶向治疗,改善肾脏和总体预后。CD19+B-Ly 再增殖先于生物复发,因此监测 CD19+B-Ly 可能成为预测复发和指导利妥昔单抗治疗的工具。