Bindu Harika M, Dogra Neeti, Makkar Jeetinder K, Bhatia Nidhi, Meena Shyam, Gupta Rajesh
Department of Anaesthesia and Intensive Care, PGIMER, Chandigarh, India.
Department of Surgical Gastroenterology, PGIMER, Chandigarh, India.
Indian J Anaesth. 2021 Aug;65(8):612-618. doi: 10.4103/ija.IJA_1508_20. Epub 2021 Aug 25.
Unpredictable difficult laryngoscopy remains a challenge for anaesthesiologists, especially in morbidly obese patients. The present study aimed to determine the efficacy of different sonographic measures as predictors of difficult laryngoscopy in morbidly obese patients undergoing elective surgery.
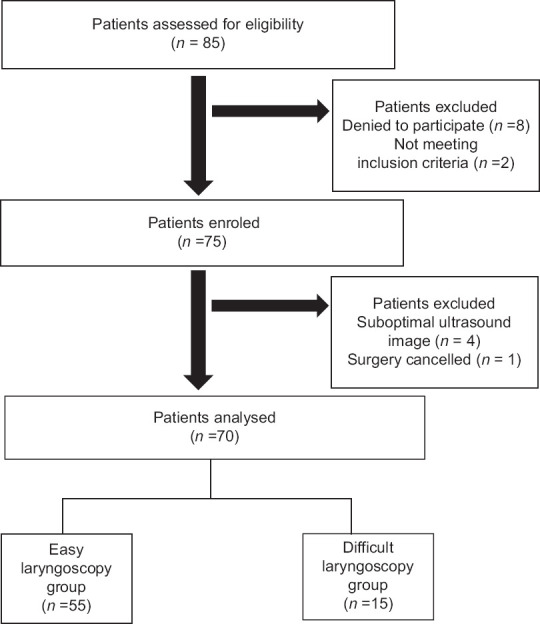
This observational study evaluated 70 morbidly obese adult patients (body mass index >35 kg/m) undergoing elective surgery under general anaesthesia with tracheal intubation. Pre-operative clinical and ultrasonographic variables (anterior condylar translation, tongue thickness, hyomental distance and oral cavity height) associated with difficult direct laryngoscopy ([Cormack Lehane (CL) grade>2]) were analysed. The primary outcome was to determine the efficacy of the above-mentioned sonographic measures as predictors of difficult laryngoscopy (CL grade >2). The secondary outcome compared ultrasonographic predictors with clinical predictors in morbidly obese patients for determining difficult direct laryngoscopy.
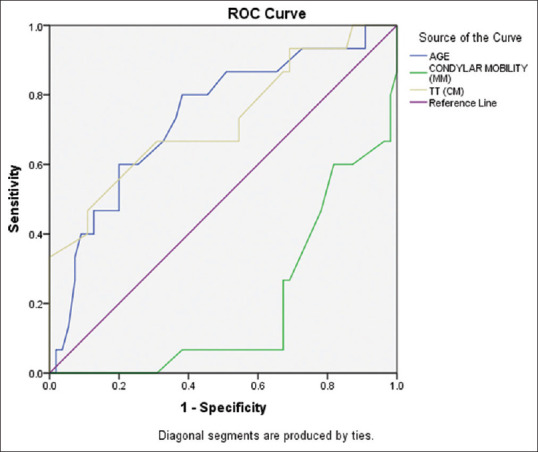
Amongst the primary outcome measures, limited condylar mobility (anterior condylar translation <9.25 mm) [odds ratio (OR) 0.3, confidence interval (CI):1.04-1.22;<0.001;area under curve (AUC):0.8] and increased tongue thickness >5.85 cm [OR: 3.2, CI: 1.05-10; < 0.04; AUC: 0.73] were two independent sonographic predictors for difficult direct laryngoscopy by multivariate logistic regression and receiver operating characteristic curve analyses in morbidly obese patients. The secondary outcome suggested that as compared to clinical predictors such as Mallampati grade and thyromental distance, ultrasonographic variables such as tongue thickness and limited condylar mobility (sensitivity: 56.4%, 70.9%, 66.7% and 93.3%, respectively) better predicted difficult direct laryngoscopy in morbidly obese patients.
Limited condylar mobility and increased tongue thickness are independent sonographic predictors of difficult direct laryngoscopy in morbidly obese patients.
难以预测的困难喉镜检查对麻醉医生来说仍然是一项挑战,尤其是在病态肥胖患者中。本研究旨在确定不同超声测量方法作为择期手术病态肥胖患者困难喉镜检查预测指标的有效性。
本观察性研究评估了70例接受全身麻醉气管插管择期手术的病态肥胖成年患者(体重指数>35kg/m²)。分析了与困难直接喉镜检查([Cormack Lehane(CL)分级>2级])相关的术前临床和超声变量(髁突前移、舌厚度、颏下距离和口腔高度)。主要结局是确定上述超声测量方法作为困难喉镜检查(CL分级>2级)预测指标的有效性。次要结局是比较病态肥胖患者中超声预测指标与临床预测指标对困难直接喉镜检查的诊断效能。
在主要结局指标中,髁突活动受限(髁突前移<9.25mm)[优势比(OR)0.3,置信区间(CI):1.04 - 1.22;P<0.001;曲线下面积(AUC):0.8]和舌厚度增加>5.85cm[OR:3.2,CI:1.05 - 10;P<0.04;AUC:0.73]是通过多因素逻辑回归和受试者工作特征曲线分析得出的病态肥胖患者困难直接喉镜检查的两个独立超声预测指标。次要结局表明,与Mallampati分级和甲颏距离等临床预测指标相比,舌厚度和髁突活动受限等超声变量(敏感性分别为56.4%、70.9%、66.7%和93.3%)能更好地预测病态肥胖患者的困难直接喉镜检查。
髁突活动受限和舌厚度增加是病态肥胖患者困难直接喉镜检查的独立超声预测指标。