Department of Nutrition and Food Hygiene, School of Public Health, Capital Medical University, 100069, Beijing, P.R. China.
FuXing Hospital, Capital Medical University, 100045, Beijing, P.R. China.
Lipids Health Dis. 2021 Sep 29;20(1):119. doi: 10.1186/s12944-021-01549-y.
Blood lipid increases during gestation are considered a physiological adaption, and decrease after delivery. However, some adverse pregnancy outcomes are thought to be related to gestational lipid levels. Therefore, it is necessary to have a reference range for lipid changes during gestation. The present study aims to describe triglyceride (TG) changes during pregnancy and 42 days postpartum and to find cut-off points for TG levels during the first, second, and third trimesters.
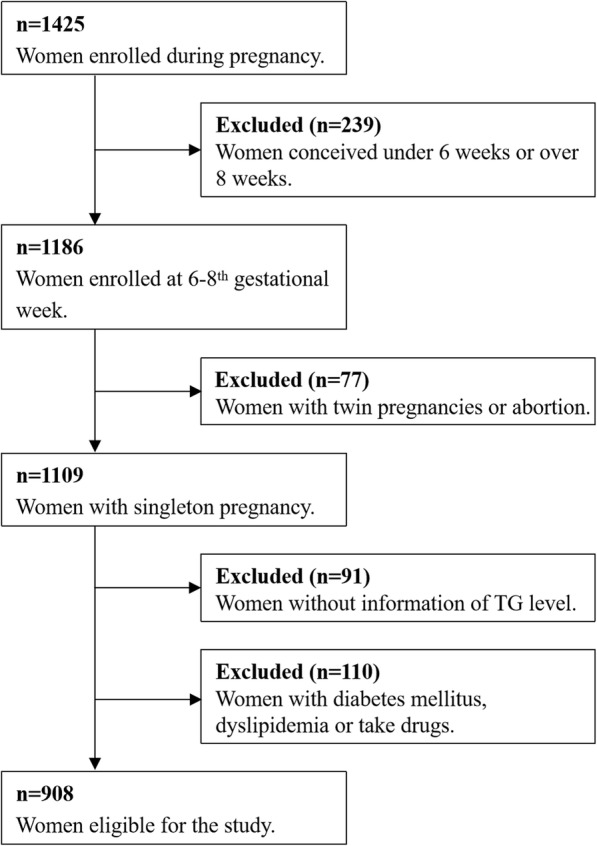
A total of 908 pregnant women were followed from recruitment to 42 days postpartum, and their serum lipids were collected at gestational weeks 6-8, 16, 24, and 36 and 42 days postpartum. The major outcome was postpartum hypertriglyceridemia. The association between gestational and postpartum TG levels was analysed by stepwise multiple linear regression. A two-stage approach including a linear mixed-effect model and linear or logistic regression was conducted to explore the contribution of the changes in TG over time in pregnancy to postpartum hypertriglyceridemia. Logistic regression was constructed to examine the association between gestational TG levels and postpartum hypertriglyceridemia. Cut-off points were calculated by receiver operating characteristic (ROC) curves.
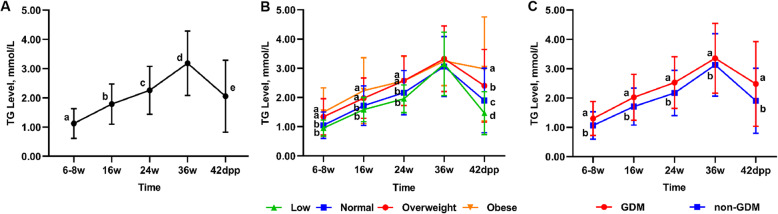
There was a tendency for serum TG to increase with gestational age and decrease at 42 days postpartum. Prepregnancy overweight, obesity, and GDM intensified this elevation. Higher TG levels at gestational weeks 6-8, 16, 24, and 36 were positively associated with a higher risk of postpartum hypertriglyceridemia [OR 4.962, 95 % CI (3.007-8.189); OR 2.076, 95 % CI (1.303-3.309); OR 1.563, 95 % CI (1.092-2.236); and OR 1.534, 95 % CI (1.208-1.946), respectively]. The trend of the change in TG over time was positively associated with the TG level and risk of postpartum hypertriglyceridemia [OR 11.660, 95 % CI (6.018-22.591)]. Based on ROC curves, the cut-off points of serum TG levels were 1.93, 2.35, and 3.08 mmol/L at gestational weeks 16, 24, and 36, respectively. Stratified analysis of prepregnancy body mass index (pre-BMI) and GDM showed that higher gestational TG was a risk factor for postpartum hypertriglyceridemia in women with normal pre-BMI and without GDM.
Gestational TG and its elevation were risk and predictive factors of postpartum hypertriglyceridemia, especially in pregnant women with normal pre-BMI or without GDM.
孕期血脂升高被认为是一种生理适应,分娩后会降低。然而,一些不良的妊娠结局被认为与妊娠期间的血脂水平有关。因此,有必要为孕期血脂变化提供参考范围。本研究旨在描述孕期和产后 42 天甘油三酯(TG)的变化,并找到孕期第一、二、三产前 TG 水平的截断值。
共随访 908 名孕妇,从招募到产后 42 天,在妊娠 6-8 周、16 周、24 周和 36 周及产后 42 天收集血清脂质。主要结局为产后高甘油三酯血症。采用逐步多元线性回归分析妊娠和产后 TG 水平之间的关系。采用线性混合效应模型和线性或逻辑回归的两阶段方法,探讨孕期 TG 随时间变化对产后高甘油三酯血症的影响。构建逻辑回归模型,检验妊娠 TG 水平与产后高甘油三酯血症的关系。通过受试者工作特征(ROC)曲线计算截断值。
血清 TG 随妊娠周数增加而升高,产后 42 天下降。妊娠前超重、肥胖和 GDM 使这种升高加剧。妊娠 6-8 周、16 周、24 周和 36 周 TG 水平较高与产后高甘油三酯血症的风险增加呈正相关[OR 4.962,95%CI(3.007-8.189);OR 2.076,95%CI(1.303-3.309);OR 1.563,95%CI(1.092-2.236);OR 1.534,95%CI(1.208-1.946)]。TG 随时间的变化趋势与产后高甘油三酯血症的 TG 水平和风险呈正相关[OR 11.660,95%CI(6.018-22.591)]。基于 ROC 曲线,血清 TG 水平的截断值分别为妊娠 16 周 1.93mmol/L、24 周 2.35mmol/L 和 36 周 3.08mmol/L。妊娠前 BMI(pre-BMI)和 GDM 的分层分析显示,对于 BMI 正常且无 GDM 的孕妇,较高的妊娠 TG 是产后高甘油三酯血症的危险因素。
妊娠 TG 及其升高是产后高甘油三酯血症的风险和预测因素,尤其是在 BMI 正常或无 GDM 的孕妇中。