Yang James Chih-Hsin, Reckamp Karen L, Kim Young-Chul, Novello Silvia, Smit Egbert F, Lee Jong-Seok, Su Wu-Chou, Akerley Wallace L, Blakely Collin M, Groen Harry J M, Bazhenova Lyudmila, Carcereny Costa Enric, Chiari Rita, Hsia Te-Chun, Golsorkhi Tony, Despain Darrin, Shih Danny, Popat Sanjay, Wakelee Heather
Department of Oncology, National Taiwan University Hospital, Taipei City, Republic of China.
Department of Medical Oncology, Cedars-Sinai Medical Center, Los Angeles, California.
JTO Clin Res Rep. 2020 Oct 26;2(2):100114. doi: 10.1016/j.jtocrr.2020.100114. eCollection 2021 Feb.
The TIGER-3 (NCT02322281) study was initiated to compare the efficacy and safety of rociletinib, a third-generation EGFR tyrosine kinase inhibitor (TKI) that targets T790M and common -activating mutations, versus chemotherapy in patients with NSCLC who progressed on first- or second-generation EGFR TKIs.
Patients with advanced or metastatic -mutated NSCLC with disease progression on standard therapy (previous EGFR TKI and platinum-based chemotherapy) were randomized to oral rociletinib (500 or 625 mg twice daily) or single-agent chemotherapy (pemetrexed, gemcitabine, docetaxel, or paclitaxel).
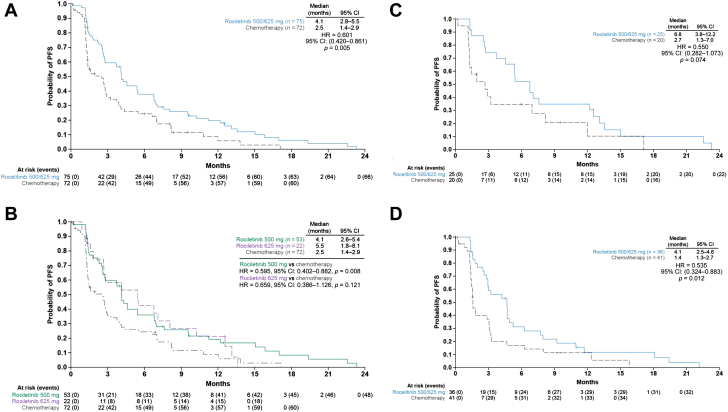
Enrollment was halted when rociletinib development was discontinued in 2016. Of 149 enrolled patients, 75 were randomized to rociletinib (n = 53: 500 mg twice daily; n = 22: 625 mg twice daily) and 74 to chemotherapy. The median investigator-assessed progression-free survival (PFS) was 4.1 months (95% confidence interval [CI]: 2.6-5.4) in the rociletinib 500-mg group and 5.5 months (95% CI: 1.8-8.1) in the 625-mg group versus 2.5 months (95% CI: 1.4-2.9) in the chemotherapy group. An improved PFS was observed in patients with T790M-positive NSCLC treated with rociletinib (n = 25; 500 mg and 625 mg twice daily) versus chemotherapy (n = 20; 6.8 versus 2.7 mo; hazard ratio = 0.55, 95% CI: 0.28-1.07, = 0.074). Grade 3 or higher hyperglycemia (24.0%), corrected QT prolongation (6.7%), diarrhea (2.7%), and vomiting (1.3%) were more frequent with rociletinib than chemotherapy (0%, 0%, 1.4%, and 0%, respectively).
Rociletinib had a more favorable median PFS versus chemotherapy but had higher rates of hyperglycemia and corrected QT prolongation in patients with advanced -mutated NSCLC who progressed on previous EGFR TKI. Incomplete enrollment prevented evaluation of the primary efficacy end point.
启动TIGER-3(NCT02322281)研究,以比较rociletinib(一种靶向T790M和常见激活突变的第三代表皮生长因子受体酪氨酸激酶抑制剂(TKI))与化疗在第一代或第二代表皮生长因子受体TKI治疗后病情进展的非小细胞肺癌患者中的疗效和安全性。
标准治疗(既往表皮生长因子受体TKI和铂类化疗)后病情进展的晚期或转移性突变非小细胞肺癌患者被随机分为口服rociletinib(500或625毫克,每日两次)或单药化疗(培美曲塞、吉西他滨、多西他赛或紫杉醇)。
2016年rociletinib研发终止时,研究入组停止。在149例入组患者中,75例被随机分配至rociletinib组(n = 53:500毫克,每日两次;n = 22:625毫克,每日两次),74例被分配至化疗组。研究者评估的中位无进展生存期(PFS)在rociletinib 500毫克组为4.1个月(95%置信区间[CI]:2.6 - 5.4),625毫克组为5.5个月(95% CI:1.8 - 8.1),而化疗组为2.5个月(95% CI:1.4 - 2.9)。在接受rociletinib治疗的T790M阳性非小细胞肺癌患者(n = 25;500毫克和625毫克,每日两次)中观察到PFS有所改善,与化疗组(n = 20;分别为6.8个月和2.7个月;风险比 = 0.55,95% CI:0.28 - 1.07,P = 0.074)相比。与化疗相比(分别为0%、0%、1.4%和0%),rociletinib治疗组3级或更高等级高血糖(24.0%)、校正QT间期延长(6.7%)、腹泻(2.7%)和呕吐(1.3%)更为常见。
对于既往表皮生长因子受体TKI治疗后病情进展的晚期突变非小细胞肺癌患者,rociletinib的中位PFS比化疗更有利,但高血糖和校正QT间期延长的发生率更高。入组不完全妨碍了对主要疗效终点的评估。