Hall R, Mitchell L, Sachdeva J
Devon Partnership Trust, UK.
Plymouth Hospitals Trust, UK.
BJPsych Open. 2021 Oct 1;7(6):e184. doi: 10.1192/bjo.2021.1022.
UK adult gender identity clinics (GICs) are implementing a new streamlined service model. However, there is minimal evidence from these services underpinning this. It is also unknown how many service users subsequently 'detransition'.
To describe service users' access to care and patterns of service use, specifically, interventions accessed, reasons for discharge and re-referrals; to identify factors associated with access; and to quantify 'detransitioning'.
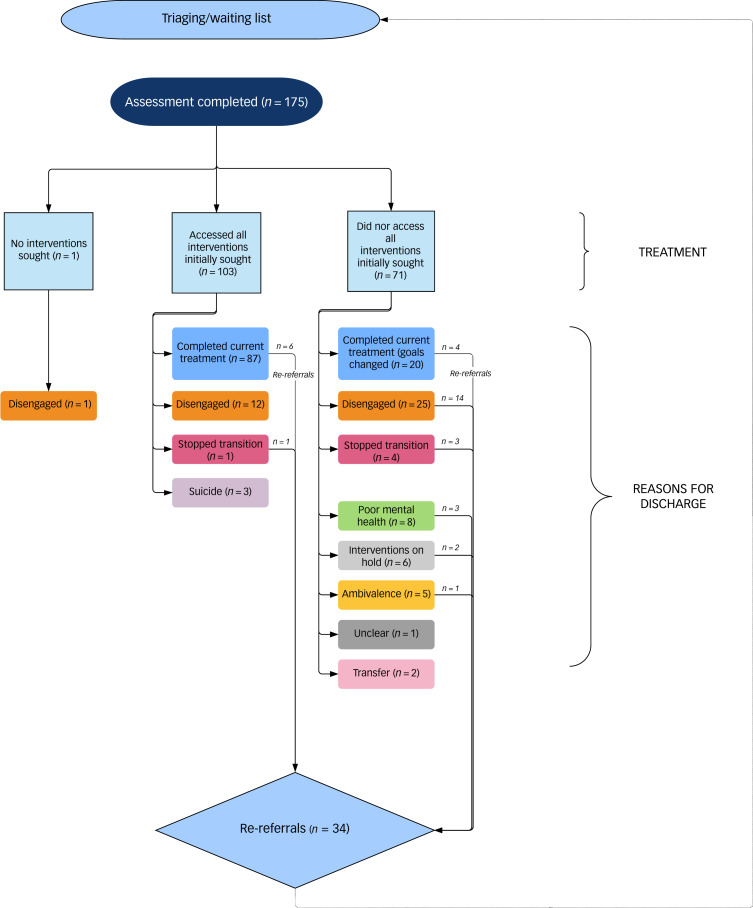
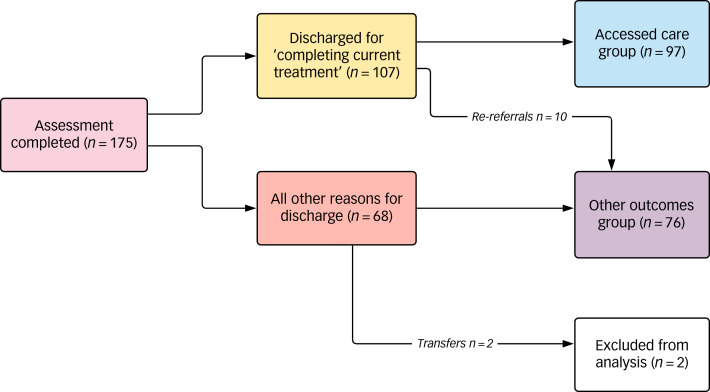
A retrospective case-note review was performed as a service evaluation for 175 service users consecutively discharged by a tertiary National Health Service adult GIC between 1 September 2017 and 31 August 2018. Descriptive statistics were used for rates of accessing interventions sought, reasons for discharge, re-referral and frequency of detransitioning. Using multivariate analysis, we sought associations between several variables and 'accessing care' or 'other outcome'.
The treatment pathway was completed by 56.1%. All interventions initially sought were accessed by 58%; 94% accessed hormones but only 47.7% accessed gender reassignment surgery; 21.7% disengaged; and 19.4% were re-referred. Multivariate analysis identified coexisting neurodevelopmental disorders (odds ratio [OR] = 5.7, 95% CI = 1.7-19), previous adverse childhood experiences (ACEs) per reported ACE (OR = 1.5, 95% CI = 1.1-1.9), substance misuse during treatment (OR = 4.3, 95% CI = 1.1-17.6) and mental health concerns during treatment (OR = 2.2, 95% CI 1.1-4.4) as independently associated with accessing care. Twelve people (6.9%) met our case definition of detransitioning.
Service users may have unmet needs. Neurodevelopmental disorders or ACEs suggest complexity requiring consideration during the assessment process. Managing mental ill health and substance misuse during treatment needs optimising. Detransitioning might be more frequent than previously reported.
英国成人性别认同诊所(GICs)正在实施一种新的简化服务模式。然而,这些服务中几乎没有证据支持这一点。同样未知的是,有多少服务使用者随后“转回原性别”。
描述服务使用者获得护理的情况和服务使用模式,具体而言,包括所接受的干预措施、出院原因和再次转诊情况;确定与获得护理相关的因素;并对“转回原性别”进行量化。
对一家三级国民保健服务成人GIC在2017年9月1日至2018年8月31日期间连续出院的175名服务使用者进行回顾性病例记录审查,作为一项服务评估。使用描述性统计来分析寻求干预措施的比例、出院原因、再次转诊情况以及转回原性别的频率。通过多变量分析,我们寻找几个变量与“获得护理”或“其他结果”之间的关联。
56.1%的人完成了治疗路径。最初寻求的所有干预措施中,58%的人获得了;94%的人接受了激素治疗,但只有47.7%的人接受了性别重置手术;21.7%的人退出了;19.4%的人被再次转诊。多变量分析确定,并存的神经发育障碍(优势比[OR]=5.7,95%置信区间[CI]=1.7-19)、每报告一次不良童年经历(ACEs)(OR=1.5,95%CI=1.1-1.9)、治疗期间药物滥用(OR=4.3,95%CI=1.1-17.6)以及治疗期间的心理健康问题(OR=2.2,95%CI 1.1-4.4)与获得护理独立相关。12人(6.9%)符合我们对转回原性别的病例定义。
服务使用者可能有未满足的需求。神经发育障碍或ACEs表明情况复杂,在评估过程中需要加以考虑。治疗期间对心理健康和药物滥用的管理需要优化。转回原性别的情况可能比之前报告的更频繁。