Tydings Caitlin, Yarmolenko Pavel, Bornhorst Miriam, Dombi Eva, Myseros John, Keating Robert, Bost James, Sharma Karun, Kim AeRang
Center for Cancer and Blood Disorders, Children's National Hospital, Washington, District of Columbia, USA.
Sheikh Zayed Institute for Pediatric Surgical Innovation, Children's National Hospital, Washington, District of Columbia, USA.
Neurooncol Adv. 2021 Aug 18;3(1):vdab116. doi: 10.1093/noajnl/vdab116. eCollection 2021 Jan-Dec.
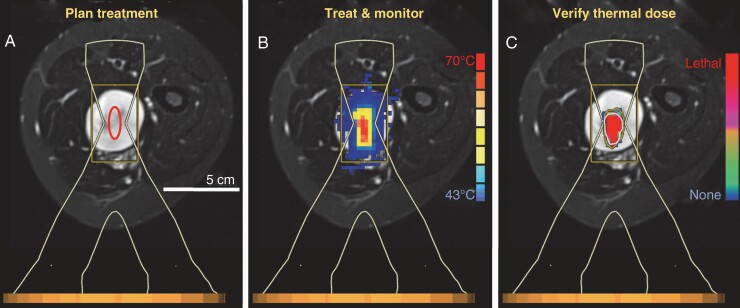
Patients with Neurofibromatosis Type 1 (NF1) and plexiform neurofibromas (PN) often have radiographically diagnosed distinct nodular lesions (DNL) which can cause pain and weakness. Magnetic resonance-guided high intensity focused ultrasound (MR-HIFU) can precisely and accurately deliver heat to thermally ablate target tissue. The aim of this study is to evaluate whole-body MRIs from patients with NF1 and DNL, applying volumetrics and a consistent treatment planning approach to determine the feasibility of MR-HIFU ablation of DNL.
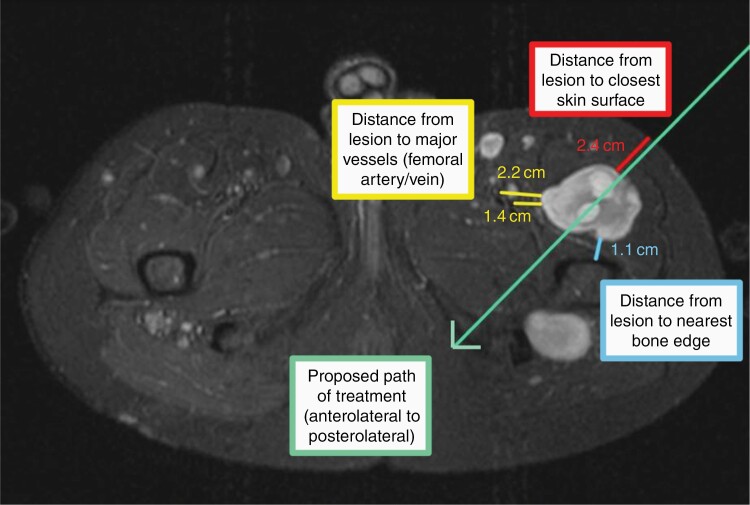
A retrospective review of whole-body MRI scans from patients with NF1 and PN from CNH and NCI was performed. DNL are defined as lesions >3 cm, distinct from PN and lacking the "central dot" feature. Criteria for MR-HIFU thermal ablation include target location 1-8 cm from skin surface; >1 cm from visible plexus, spinal canal, bladder, bowel, physis; and ability to ablate ≥50% of lesion volume. Lesions in skull and vertebral body were excluded.
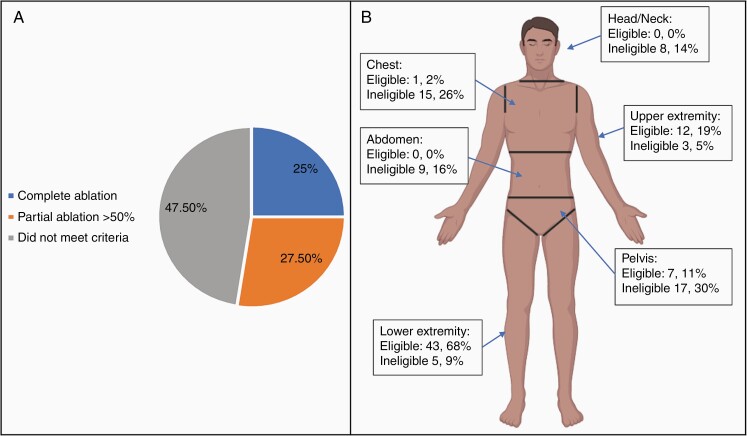
In 26 patients, 120 DNL were identified. The majority of DNL were located in an extremity (52.5%). Other sites included head/neck (7%), chest (13%), and abdomen/pelvis (28%). The predefined HIFU ablation criteria was not met for 47.5% of lesions ( = 57). The main limitation was proximity to a vital structure or organ (79%). Complete and partial HIFU ablation was feasible for 25% and 27.5% of lesions, respectively.
Based on imaging review of lesion location, technical considerations and ability to target lesions, thermal ablation with MR-HIFU may be a feasible noninvasive alternative for symptom management in patients with NF1 and symptomatic DNL.
1型神经纤维瘤病(NF1)和丛状神经纤维瘤(PN)患者常出现经影像学诊断的明显结节性病变(DNL),这些病变可导致疼痛和无力。磁共振引导下高强度聚焦超声(MR-HIFU)能够精确地将热量传递至目标组织以进行热消融。本研究旨在评估NF1和DNL患者的全身磁共振成像(MRI),采用体积测量法和一致的治疗计划方法来确定MR-HIFU消融DNL的可行性。
对来自CNH和NCI的NF1和PN患者的全身MRI扫描进行回顾性分析。DNL定义为直径大于3 cm、与PN不同且缺乏“中心点”特征的病变。MR-HIFU热消融的标准包括目标位于距皮肤表面1-8 cm处;距可见神经丛、椎管、膀胱、肠道、骨骺大于1 cm;且能够消融≥50%的病变体积。颅骨和椎体的病变被排除。
在26例患者中,共识别出120个DNL。大多数DNL位于四肢(52.5%)。其他部位包括头颈部(7%)、胸部(13%)和腹部/骨盆(28%)。47.5%的病变(n = 57)不符合预先设定的HIFU消融标准。主要限制因素是靠近重要结构或器官(79%)。分别有25%和27.5%的病变可行完全和部分HIFU消融。
基于对病变位置的影像学评估、技术考量以及靶向病变的能力,MR-HIFU热消融可能是NF1和有症状DNL患者症状管理的一种可行的非侵入性替代方法