Harvard Medical School, Boston, Massachusetts; Department of Ophthalmology, Massachusetts Eye and Ear Infirmary, Boston, Massachusetts.
University of Michigan Medical School, Ann Arbor, Michigan; Harvard T.H. Chan School of Public Health, Boston, Massachusetts.
Ophthalmology. 2022 Apr;129(4):397-405. doi: 10.1016/j.ophtha.2021.09.022. Epub 2021 Oct 6.
Evaluate differences in eye care utilization among patients with glaucoma by race and socioeconomic status (SES).
Retrospective cohort study.
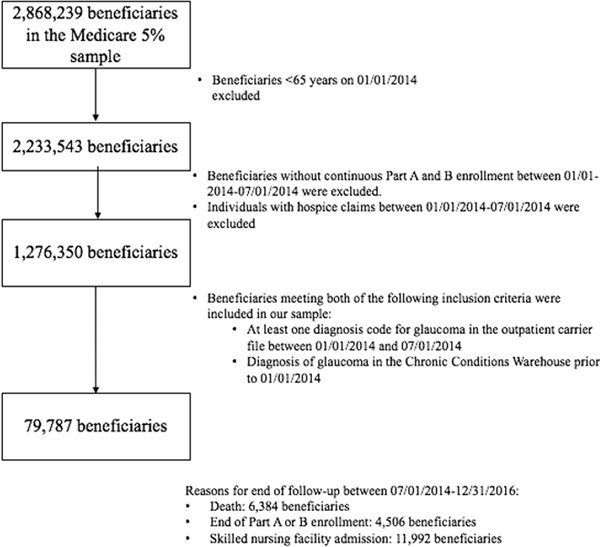
Representative 5% sample of Medicare beneficiaries aged > 65 years with continuous part A/B enrollment between January 1, 2014, and July 1, 2014, at least 1 diagnosis code for glaucoma within that period, and a glaucoma diagnosis in the Chronic Conditions Warehouse before January 1, 2014.
The following race/ethnicity categories were defined in our cohort: non-Hispanic White, Black/African American, Hispanic, and Asian/Pacific Islander. Low SES was defined as having 2 or more enrollment-based low-income indicators (dual eligibility for Medicare/Medicaid, Part D limited income subsidies, and eligibility for Part A and B State buy-in). Negative binomial regression analyses were carried out to compare relative rate ratios (RRs) of eye care utilization among racial groups stratified by low and non-low SES.
Measured from July 1, 2014, to December 31, 2016: eye examinations and eye care-related office visits; eye care-related inpatient and emergency department (ED) encounters; eye care-related nursing home and home-visit encounters; visual field and retinal nerve fiber OCT tests; glaucoma lasers and surgeries.
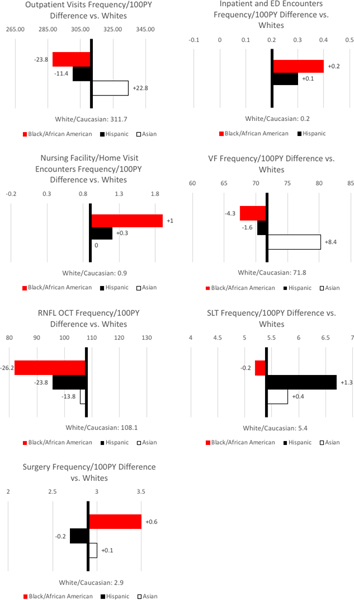
Among 78 526 participants with glaucoma, mean age was 79.1 years (standard deviation, 7.9 years), 60.9% were female, 78.4% were non-Hispanic White, and 13.8% met enrollment-based criteria for low-SES. Compared with White beneficiaries, Blacks had lower counts of outpatient visits (RR, 0.92; 95% confidence interval [CI], 0.90-0.93), visual field (VF) tests (RR, 0.92; 95% CI, 0.90-0.94), but more inpatient/ED encounters (RR, 2.42; 95% CI, 1.55-3.78) and surgeries (RR, 1.14; 95% CI, 1.03-1.27). Hispanics had fewer outpatient visits (RR, 0.97; 95% CI, 0.95-0.98) and retinal nerve fiber layer (RNFL) OCT tests (RR, 0.89; 95% CI, 0.86-0.93), but more inpatient/ED encounters (RR, 2.32; 95% CI, 1.18-4.57) and selective laser trabeculoplasty (SLT) (RR, 1.25; 95% CI, 1.11-1.42) versus non-Hispanic Whites. In the non-low SES group, Black versus White disparities persisted in outpatient visits (RR, 0.93; 95% CI, 0.92-0.95), VF (RR, 0.96; 95% CI, 0.94-0.98), RNFL OCT (RR, 0.81; 95% CI, 0.78-0.83), and inpatient/ED encounters (RR, 2.57; 95% CI, 1.55-4.26).
Disparities were found in eye care utilization among Black and Hispanic patients with glaucoma. These differences persisted among Blacks after stratification by SES, suggesting that systemic racism may be an independent driver in this population.
评估不同种族和社会经济地位(SES)的青光眼患者的眼科护理利用差异。
回顾性队列研究。
代表 2014 年 1 月 1 日至 7 月 1 日期间 Medicare 受益人的连续 A/B 部分注册的 5%的样本,在该期间内至少有 1 个青光眼诊断代码,并且在 2014 年 1 月 1 日之前在慢性疾病仓库中有青光眼诊断。
我们的队列中定义了以下种族/族裔类别:非西班牙裔白人、黑人和非裔美国人、西班牙裔和亚洲/太平洋岛民。低 SES 定义为具有 2 个或更多基于登记的低收入指标(Medicare/Medicaid 双重资格、部分 D 有限收入补贴以及部分 A 和 B 州参保资格)。进行负二项回归分析,以比较低 SES 和非低 SES 种族群体中眼科护理利用的相对比率(RR)。
从 2014 年 7 月 1 日至 2016 年 12 月 31 日测量:眼部检查和眼科相关门诊就诊;眼科相关住院和急诊(ED)就诊;眼科相关疗养院和家庭就诊;视野和视网膜神经纤维 OCT 检查;青光眼激光和手术。
在 78526 名患有青光眼的参与者中,平均年龄为 79.1 岁(标准差,7.9 岁),60.9%为女性,78.4%为非西班牙裔白人,13.8%符合基于登记的低 SES 标准。与白人受益相比,黑人的门诊就诊次数较少(RR,0.92;95%置信区间[CI],0.90-0.93),视野(VF)测试(RR,0.92;95%CI,0.90-0.94),但住院/ED 就诊次数(RR,2.42;95%CI,1.55-3.78)和手术次数(RR,1.14;95%CI,1.03-1.27)更多。西班牙裔人的门诊就诊次数(RR,0.97;95%CI,0.95-0.98)和视网膜神经纤维层(RNFL)OCT 检查次数(RR,0.89;95%CI,0.86-0.93)较少,但住院/ED 就诊次数(RR,2.32;95%CI,1.18-4.57)和选择性激光小梁成形术(SLT)(RR,1.25;95%CI,1.11-1.42)较非西班牙裔白人更多。在非低 SES 组中,黑人与白人在门诊就诊(RR,0.93;95%CI,0.92-0.95)、VF(RR,0.96;95%CI,0.94-0.98)、RNFL OCT(RR,0.81;95%CI,0.78-0.83)和住院/ED 就诊(RR,2.57;95%CI,1.55-4.26)方面仍存在差异。
在患有青光眼的黑人和西班牙裔患者中发现了眼科护理利用方面的差异。这些差异在 SES 分层后仍存在于黑人中,表明系统性种族主义可能是该人群的一个独立驱动因素。