Friedrich Michael, Kühn Thorsten, Janni Wolfgang, Müller Volkmar, Banys-Pachulowski Maggie, Kolberg-Liedtke Cornelia, Jackisch Christian, Krug David, Albert Ute-Susann, Bauerfeind Ingo, Blohmer Jens, Budach Wilfried, Dall Peter, Fallenberg Eva M, Fasching Peter A, Fehm Tanja, Gerber Bernd, Gluz Oleg, Hanf Volker, Harbeck Nadia, Heil Jörg, Huober Jens, Kreipe Hans-Heinrich, Kümmel Sherko, Loibl Sibylle, Lüftner Diana, Lux Michael Patrick, Maass Nicolai, Möbus Volker, Mundhenke Christoph, Nitz Ulrike, Park-Simon Tjoung-Won, Reimer Toralf, Rhiem Kerstin, Rody Achim, Schmidt Marcus, Schneeweiss Andreas, Schütz Florian, Sinn Hans-Peter, Solbach Christine, Solomayer Erich-Franz, Stickeler Elmar, Thomssen Christoph, Untch Michael, Witzel Isabell, Wöckel Achim, Thill Marc, Ditsch Nina
Klinik für Frauenheilkunde und Geburtshilfe, HELIOS Klinikum Krefeld, Krefeld, Germany.
Gynäkologie, Klinikum Esslingen, Esslingen, Germany.
Geburtshilfe Frauenheilkd. 2021 Oct;81(10):1112-1120. doi: 10.1055/a-1499-8431. Epub 2021 Oct 6.
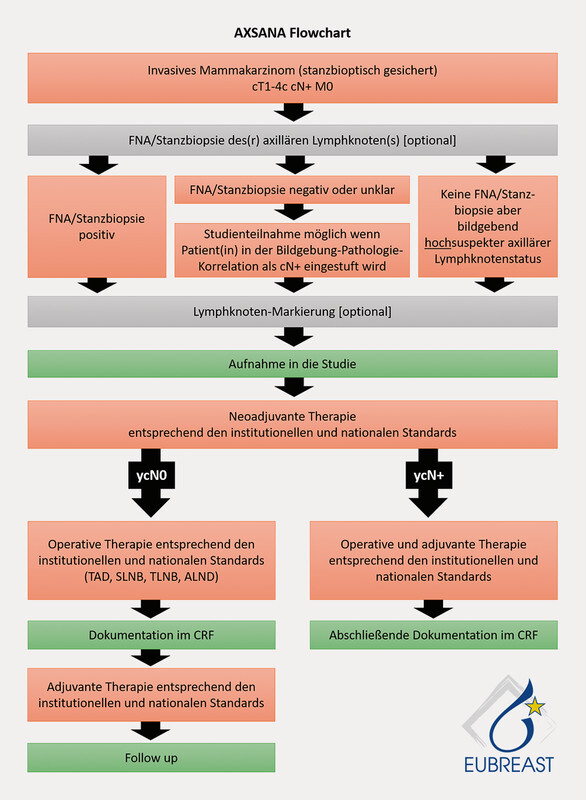
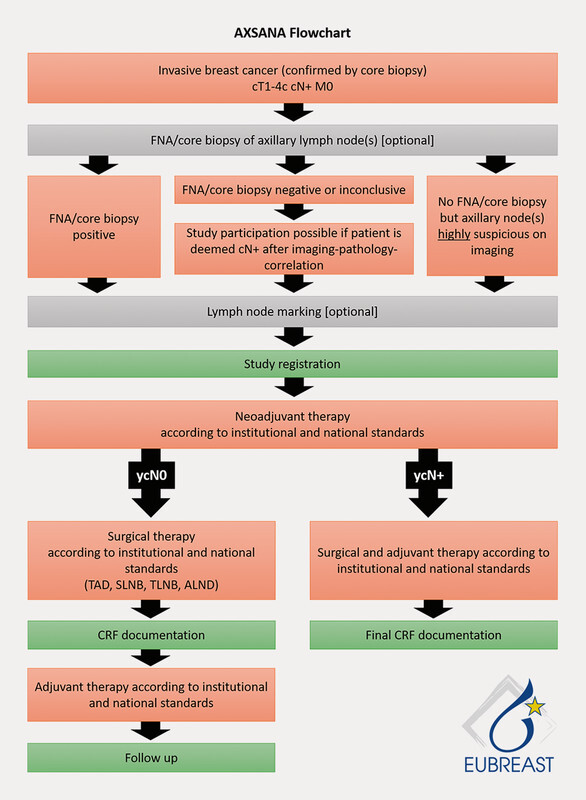
For many decades, the standard procedure to treat breast cancer included complete dissection of the axillary lymph nodes. The aim was to determine histological node status, which was then used as the basis for adjuvant therapy, and to ensure locoregional tumour control. In addition to the debate on how to optimise the therapeutic strategies of systemic treatment and radiotherapy, the current discussion focuses on improving surgical procedures to treat breast cancer. As neoadjuvant chemotherapy is becoming increasingly important, the surgical procedures used to treat breast cancer, whether they are breast surgery or axillary dissection, are changing. Based on the currently available data, carrying out SLNE prior to neoadjuvant chemotherapy is not recommended. In contrast, surgical axillary management after neoadjuvant chemotherapy is considered the procedure of choice for axillary staging and can range from SLNE to TAD and ALND. To reduce the rate of false negatives during surgical staging of the axilla in pN+ stage before NACT and ycN0 after NACT, targeted axillary dissection (TAD), the removal of > 2 SLNs (SLNE, no untargeted axillary sampling), immunohistochemistry to detect isolated tumour cells and micro-metastases, and marking positive lymph nodes before NACT should be the standard approach. This most recent update on surgical axillary management describes the significance of isolated tumour cells and micro-metastasis after neoadjuvant chemotherapy and the clinical consequences of low volume residual disease diagnosed using SLNE and TAD and provides an overview of this year's AGO recommendations for surgical management of the axilla during primary surgery and in relation to neoadjuvant chemotherapy.
几十年来,治疗乳腺癌的标准程序包括腋窝淋巴结完全清扫。目的是确定组织学淋巴结状态,然后将其作为辅助治疗的基础,并确保局部区域肿瘤得到控制。除了关于如何优化全身治疗和放疗的治疗策略的争论外,目前的讨论集中在改进治疗乳腺癌的手术方法上。随着新辅助化疗变得越来越重要,用于治疗乳腺癌的手术方法,无论是乳房手术还是腋窝清扫,都在发生变化。根据目前可得的数据,不建议在新辅助化疗之前进行前哨淋巴结活检(SLNE)。相比之下,新辅助化疗后的腋窝手术处理被认为是腋窝分期的首选方法,范围可以从前哨淋巴结活检到治疗性腋窝清扫(TAD)和腋窝淋巴结清扫(ALND)。为了降低在新辅助化疗前pN+期腋窝手术分期以及新辅助化疗后ycN0期腋窝手术分期期间的假阴性率,靶向腋窝清扫(TAD)、切除>2枚前哨淋巴结(前哨淋巴结活检,不进行非靶向腋窝采样)、采用免疫组织化学检测孤立肿瘤细胞和微转移,以及在新辅助化疗前标记阳性淋巴结应作为标准方法。关于腋窝手术处理的这一最新更新描述了新辅助化疗后孤立肿瘤细胞和微转移的意义,以及使用前哨淋巴结活检和靶向腋窝清扫诊断的低体积残留疾病的临床后果,并概述了今年德国乳腺癌研究组(AGO)关于初次手术期间以及与新辅助化疗相关的腋窝手术管理的建议。