Department of Neurology, Kuang Tien General Hospital, Taichung, Taiwan.
Department of Nutrition, Hungkuang University, Taichung, Taiwan.
JAMA Netw Open. 2021 Oct 1;4(10):e2128544. doi: 10.1001/jamanetworkopen.2021.28544.
New therapeutic classes of migraine-specific treatment have been developed, including 5-hydroxytryptamine1F receptor agonists (lasmiditan) and calcitonin gene-related peptide antagonists (rimegepant and ubrogepant).
To compare outcomes associated with the use of lasmiditan, rimegepant, and ubrogepant vs triptans for acute management of migraine headaches.
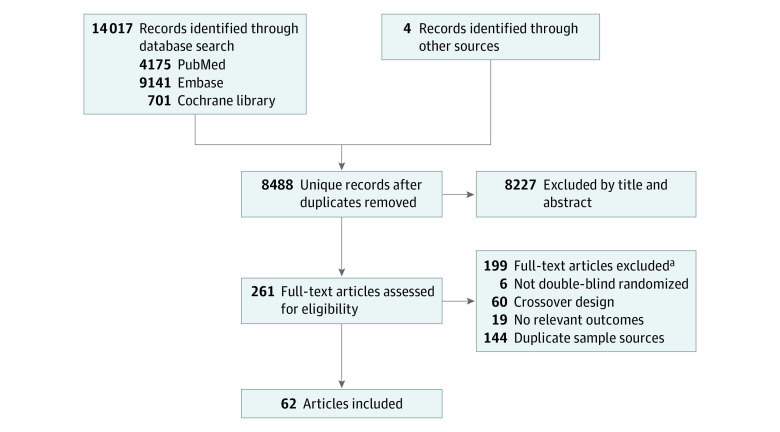
The Cochrane Register of Controlled Trials, Embase, and PubMed were searched from inception to March 5, 2020.
Double-blind randomized clinical trials examining current available migraine-specific acute treatments were included.
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline was applied to extract the data according to a predetermined list of variables of interest, and all network meta-analyses were conducted using a random-effects model.
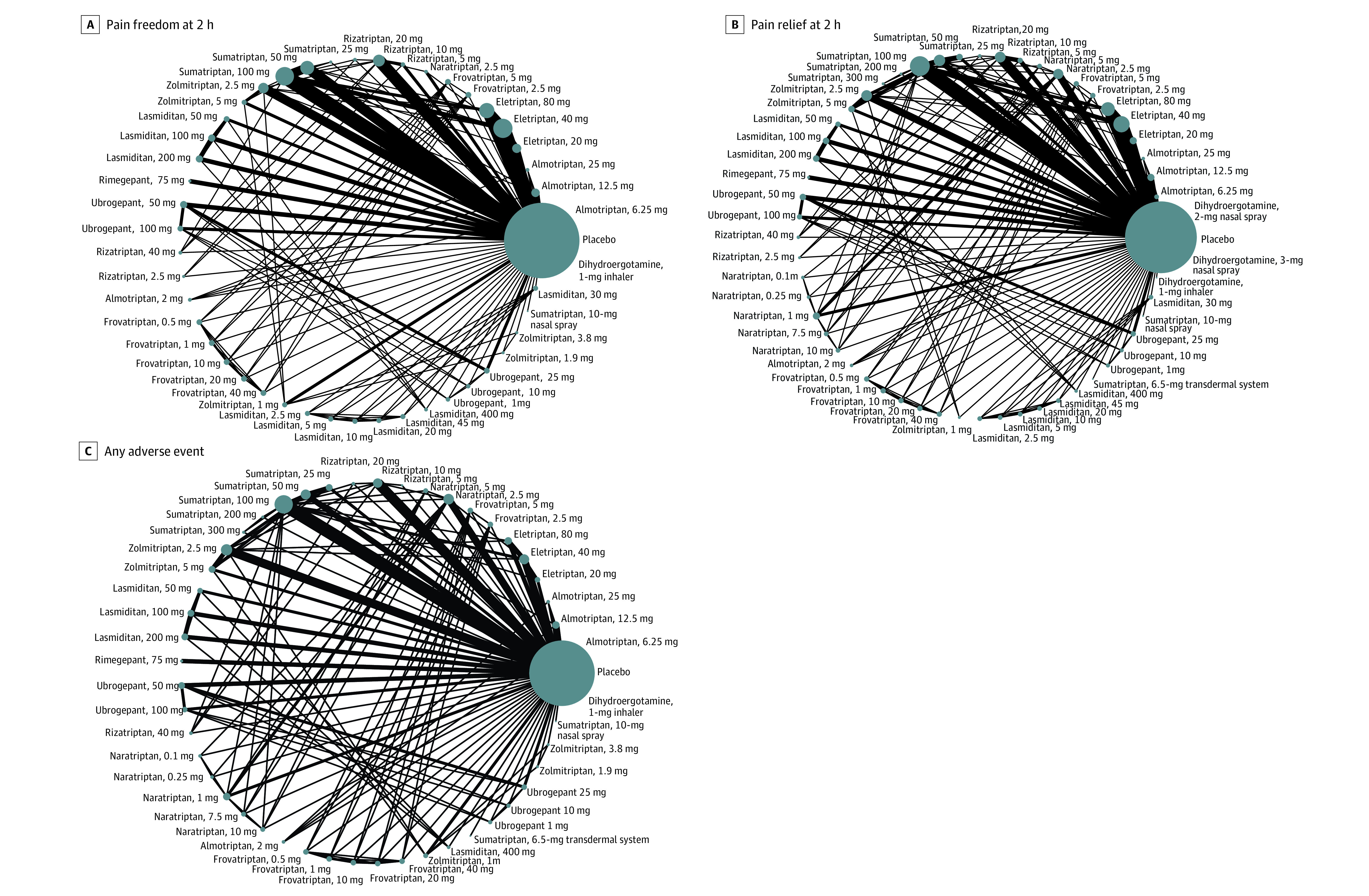
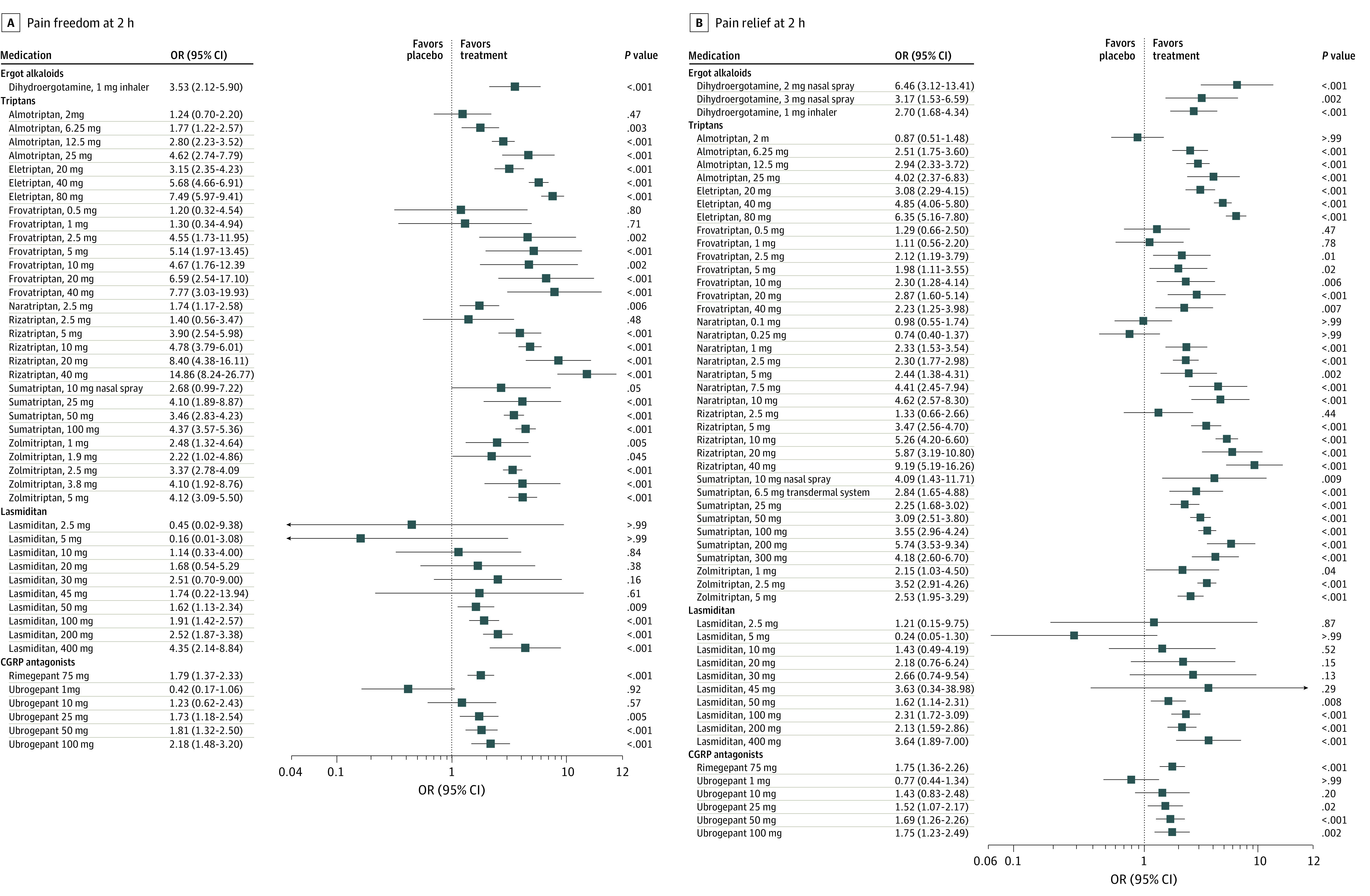
The primary outcome was the odds ratio (OR) for freedom from pain (hereafter referred to as pain freedom) at 2 hours after the dose, and the secondary outcomes were ORs for pain relief at 2 hours after the dose and any adverse events.
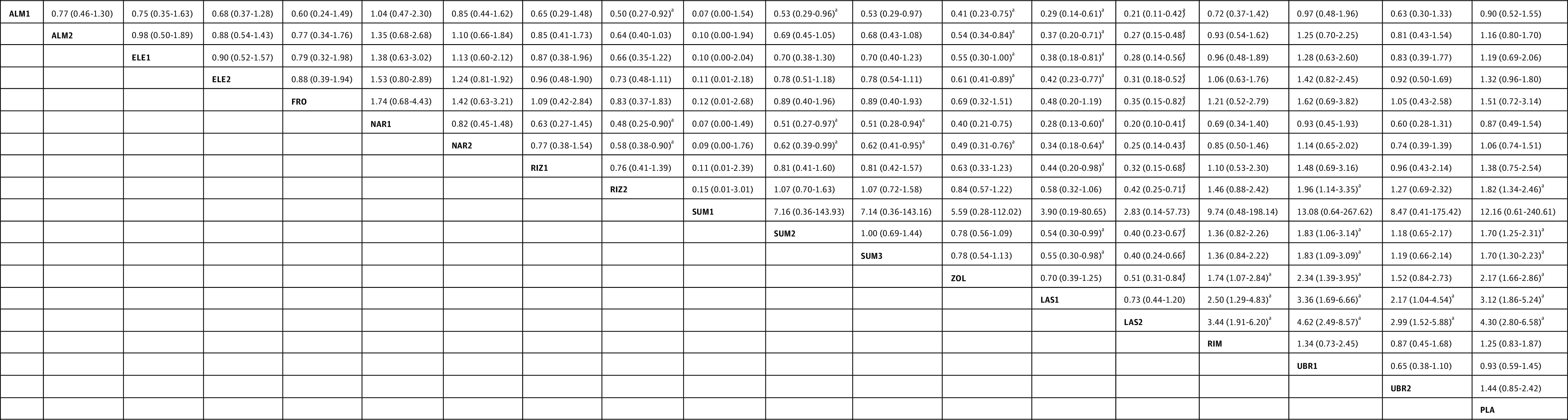
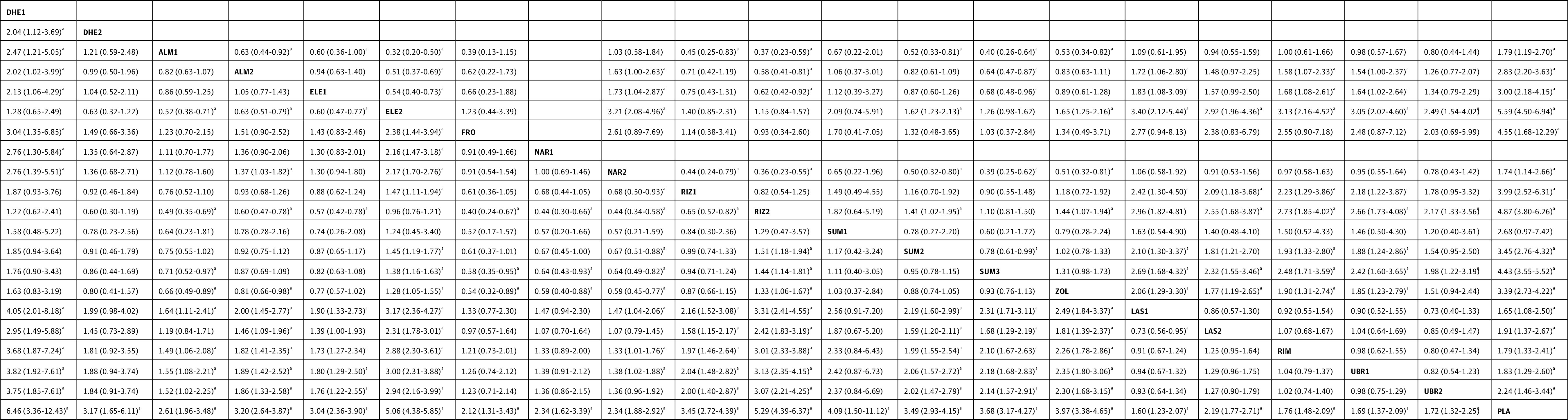
A total of 64 randomized clinical trials were included (46 442 participants; 74%-87% women; age range, 36-43 years). Most of the included treatments were associated with reduced pain at 2 hours compared with placebo. Most triptans were associated with higher ORs for pain freedom at 2 hours compared with lasmiditan (range: OR, 1.72 [95% CI, 1.06-2.80] to OR, 3.40 [95% CI, 2.12-5.44]), rimegepant (range: OR, 1.58 [95% CI, 1.07-2.33] to OR, 3.13 [95% CI, 2.16-4.52]), and ubrogepant (range: OR, 1.54 [95% CI, 1.00-2.37] to OR, 3.05 [95% CI, 2.02-4.60]). Most triptans were associated with higher ORs for pain relief at 2 hours compared with lasmiditan (range: OR, 1.46 [95% CI, 1.09-1.96] to OR, 3.31 [95% CI, 2.41-4.55]), rimegepant (range: OR, 1.33 [95% CI, 1.01-1.76] to OR, 3.01 [95% CI, 2.33-3.88]), and ubrogepant (range: OR, 1.38 [95% CI, 1.02-1.88] to OR, 3.13 [95% CI, 2.35-4.15]). The comparisons between lasmiditan, rimegepant, and ubrogepant were not statistically significant for both pain freedom and pain relief at 2 hours. Lasmiditan was associated with the highest risk of any adverse events, and certain triptans (rizatriptan, sumatriptan, and zolmitriptan) were also associated with a higher risk of any adverse events than the calcitonin gene-related peptide antagonists.
For pain freedom or pain relief at 2 hours after the dose, lasmiditan, rimegepant, and ubrogepant were associated with higher ORs compared with placebo but lower ORs compared with most triptans. However, the lack of cardiovascular risks for these new classes of migraine-specific treatments may offer an alternative to triptans.
已经开发出了新的偏头痛特异性治疗类别的药物,包括 5-羟色胺 1F 受体激动剂(拉米替坦)和降钙素基因相关肽拮抗剂(rimegepant 和 ubrogepant)。
比较拉米替坦、rimegepant 和 ubrogepant 与曲坦类药物用于偏头痛急性治疗的结果。
从成立到 2020 年 3 月 5 日,在 Cochrane 对照试验注册库、Embase 和 PubMed 上进行了检索。
纳入了关于当前可用的偏头痛特异性急性治疗的双盲随机临床试验。
按照预定的感兴趣变量列表,应用系统评价和荟萃分析的首选报告项目(PRISMA)指南提取数据,所有网络荟萃分析均采用随机效应模型进行。
主要结果是剂量后 2 小时无疼痛(以下简称疼痛缓解)的优势比(OR),次要结果是剂量后 2 小时疼痛缓解的 OR 和任何不良事件。
共纳入 64 项随机临床试验(46442 名参与者;74%-87%为女性;年龄范围 36-43 岁)。大多数纳入的治疗方法与安慰剂相比,在 2 小时内疼痛减轻。与拉米替坦相比,大多数曲坦类药物在 2 小时时疼痛缓解的 OR 更高(范围:OR,1.72[95%CI,1.06-2.80]至 OR,3.40[95%CI,2.12-5.44]),rimegepant(范围:OR,1.58[95%CI,1.07-2.33]至 OR,3.13[95%CI,2.16-4.52])和 ubrogepant(范围:OR,1.54[95%CI,1.00-2.37]至 OR,3.05[95%CI,2.02-4.60])。与拉米替坦相比,大多数曲坦类药物在 2 小时时疼痛缓解的 OR 更高(范围:OR,1.46[95%CI,1.09-1.96]至 OR,3.31[95%CI,2.41-4.55]),rimegepant(范围:OR,1.33[95%CI,1.01-1.76]至 OR,3.01[95%CI,2.33-3.88])和 ubrogepant(范围:OR,1.38[95%CI,1.02-1.88]至 OR,3.13[95%CI,2.35-4.15])。拉米替坦、rimegepant 和 ubrogepant 之间的比较在 2 小时时的疼痛缓解和疼痛缓解方面均无统计学意义。拉米替坦与任何不良事件的风险最高,某些曲坦类药物(利扎曲坦、舒马曲坦和佐米曲坦)与降钙素基因相关肽拮抗剂相比,也有更高的任何不良事件风险。
对于剂量后 2 小时的疼痛缓解或疼痛缓解,拉米替坦、rimegepant 和 ubrogepant 与安慰剂相比,OR 更高,但与大多数曲坦类药物相比,OR 较低。然而,这些新的偏头痛特异性治疗类别的药物没有心血管风险,这可能为曲坦类药物提供了替代方案。