Partners In Health-Rwanda/Inshuti Mu Buzima, Rwinkwavu, Rwanda.
Harvard Medical School, Department of Global Health and Social Medicine, Boston, Massachusetts, United States of America.
PLoS One. 2021 Oct 11;16(10):e0257917. doi: 10.1371/journal.pone.0257917. eCollection 2021.
As part of the integration of refugees into Rwanda's national hepatitis C elimination agenda, a mass screening campaign for hepatitis B (HBV) and hepatitis C (HCV) was conducted among Burundian refugees living in Mahama Camp, Eastern Rwanda. This cross-sectional survey used data from the screening campaign to report on the epidemiology of viral hepatitis in this setting.
Rapid diagnostic tests (RDTs) were used to screen for hepatitis B surface antigen (HBsAg) and hepatitis C antibody (anti-HCV) among people of ≥15years old. We calculated seroprevalence for HBsAg and anti-HCV by age and sex and also calculated age-and-sex adjusted risk ratios (ARR) for other possible risk factors.
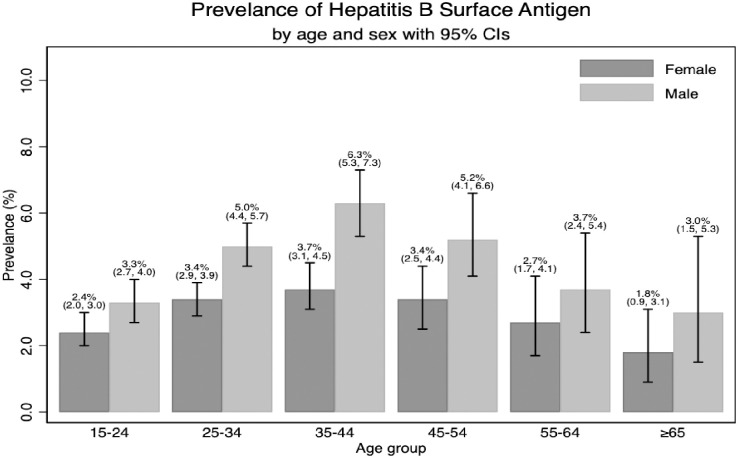
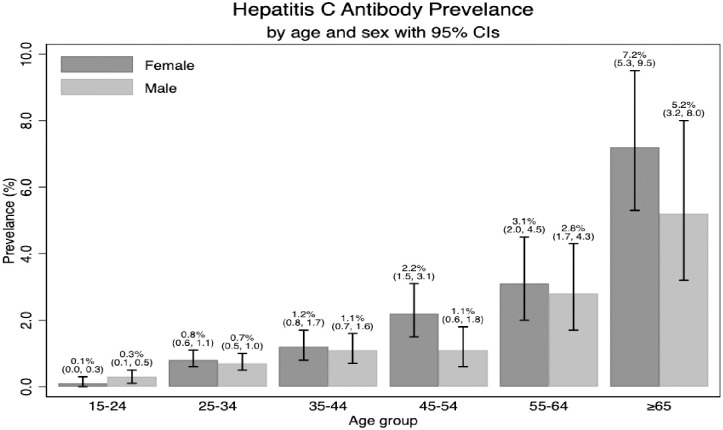
Of the 26,498 screened refugees, 1,006 (3.8%) and 297 (1.1%) tested positive for HBsAg and Anti-HCV, respectively. HBsAg was more prevalent among men than women and most common among people 25-54 years old. Anti-HCV prevalence increased with age group with no difference between sexes. After adjusting for age and sex, having a household contact with HBsAg was associated with 1.59 times higher risk of having HBsAg (95% CI: 1.27, 1.99) and having a household contact with anti-HCV was associated with 3.66 times higher risk of Anti-HCV (95% CI: 2.26, 5.93). Self-reporting having HBV, HCV, liver disease, or previously screened for HBV and HCV were significantly associated with both HBsAg and anti-HCV, but RDT-confirmed HBsAg and anti-HCV statuses were not associated with each other. Other risk factors for HBsAg included diabetes (ARR = 1.97, 95% CI: 1.08, 3.59) and family history of hepatitis B (ARR = 1.32, 95% CI: 1.11, 1.56) and for anti-HCV included heart disease (ARR = 1.91, 95% CI: 1.30, 2.80) and history of surgery (ARR = 1.70, 95% CI: 1.24, 2.32).
Sero-prevalence and risks factors for hepatitis B and C among Burundian were comparable to that in the Rwandan general population. Contact tracing among household members of identified HBsAg and anti-HCV infected case may be an effective approach to targeted hepatitis screening given the high risk among self-reported cases. Expanded access to voluntary testing may be needed to improve access to hepatitis treatment and care in other refugee settings.
作为难民融入卢旺达国家丙型肝炎消除议程的一部分,对居住在卢旺达东部马哈马难民营的布隆迪难民进行了乙型肝炎(HBV)和丙型肝炎(HCV)大规模筛查活动。这项横断面调查使用了筛查活动的数据,报告了这一环境中病毒性肝炎的流行病学情况。
对年龄在 15 岁及以上的人群使用快速诊断检测(RDT)检测乙型肝炎表面抗原(HBsAg)和丙型肝炎抗体(抗-HCV)。我们按年龄和性别计算了 HBsAg 和抗-HCV 的血清流行率,还计算了其他可能的危险因素的年龄和性别调整风险比(ARR)。
在 26498 名接受筛查的难民中,1006 人(3.8%)和 297 人(1.1%)的 HBsAg 和抗-HCV 检测结果呈阳性。HBsAg 在男性中的流行率高于女性,在 25-54 岁的人群中最为常见。抗-HCV 的流行率随年龄组而增加,男女之间没有差异。在调整年龄和性别后,与 HBsAg 家庭接触者的 HBsAg 感染风险高 1.59 倍(95%CI:1.27,1.99),与抗-HCV 家庭接触者的抗-HCV 感染风险高 3.66 倍(95%CI:2.26,5.93)。自我报告的乙型肝炎、丙型肝炎、肝病或以前筛查过乙型肝炎和丙型肝炎与 HBsAg 和抗-HCV 均显著相关,但 RDT 确认的 HBsAg 和抗-HCV 状态之间没有相关性。HBsAg 的其他危险因素包括糖尿病(ARR=1.97,95%CI:1.08,3.59)和乙型肝炎家族史(ARR=1.32,95%CI:1.11,1.56),抗-HCV 的其他危险因素包括心脏病(ARR=1.91,95%CI:1.30,2.80)和手术史(ARR=1.70,95%CI:1.24,2.32)。
布隆迪难民的乙型肝炎和丙型肝炎血清流行率和危险因素与卢旺达普通人群相当。鉴于自我报告病例中的高风险,对确定的 HBsAg 和抗-HCV 感染病例的家庭成员进行接触者追踪可能是一种针对目标的肝炎筛查的有效方法。在其他难民环境中,可能需要扩大获得自愿检测的机会,以改善获得肝炎治疗和护理的机会。