Primary Care Stratified Medicine (PRISM) Research Group, School of Medicine, University of Nottingham, Nottingham, UK
Primary Care Stratified Medicine (PRISM) Research Group, School of Medicine, University of Nottingham, Nottingham, UK.
Open Heart. 2021 Oct;8(2). doi: 10.1136/openhrt-2021-001752.
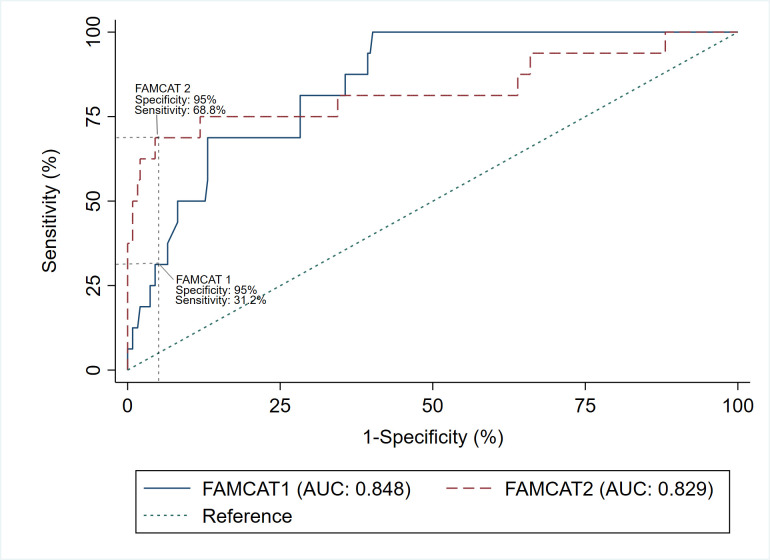
Familial hypercholesterolaemia (FH) is a common inherited disorder causing premature coronary heart disease (CHD) and death. We have developed the novel Familial Hypercholesterolaemia Case Ascertainment Tool (FAMCAT 1) case-finding algorithm for application in primary care, to improve detection of FH. The performance of this algorithm was further improved by including personal history of premature CHD (FAMCAT 2 algorithm). This study has evaluated their performance, at 95% specificity, to detect genetically confirmed FH in the general population. We also compared these algorithms to established clinical case-finding criteria.
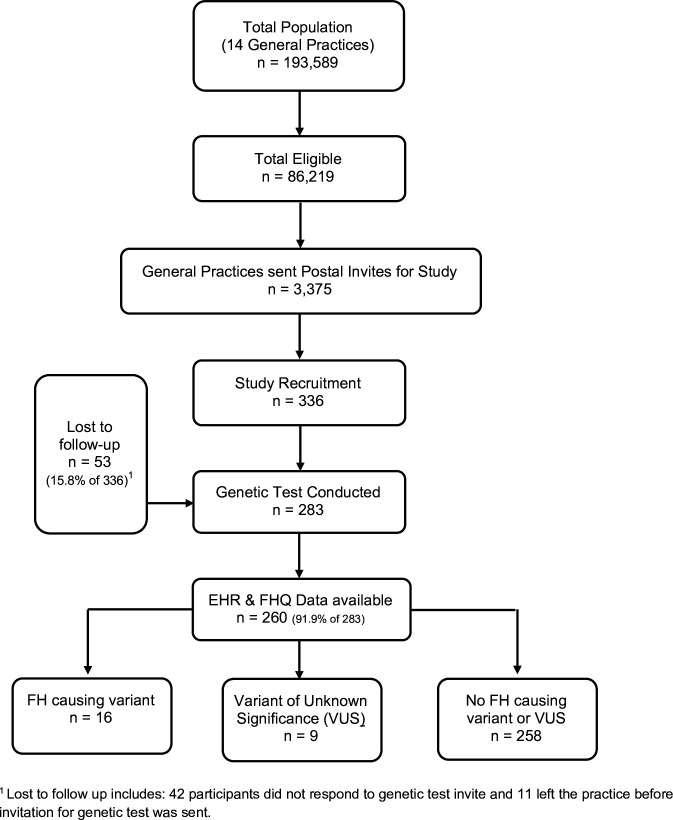
Prospective validation study, in 14 general practices, recruiting participants from the general adult population with cholesterol documented. For 260 participants with available health records, we determined possible FH cases based on FAMCAT thresholds, Dutch Lipid Clinic Network (DLCN) score, Simon-Broome criteria and recommended cholesterol thresholds (total cholesterol >9.0 mmol/L if ≥30 years or >7.5 mmol/L if <30 years), using clinical data from electronic and manual extraction of patient records and family history questionnaires. The reference standard was genetic testing. We examined detection rate (DR), sensitivity and specificity for each case-finding criteria.
At 95% specificity, FAMCAT 1 had a DR of 27.8% (95% CI 12.5% to 50.9%) with sensitivity of 31.2% (95% CI 11.0% to 58.7%); while FAMCAT 2 had a DR of 45.8% (95% CI 27.9% to 64.9%) with sensitivity of 68.8% (95% CI 41.3% to 89.0%). DLCN score ≥6 points yielded a DR of 35.3% (95% CI 17.3% to 58.7%) and sensitivity of 37.5% (95% CI 15.2% to 64.6%). Using recommended cholesterol thresholds resulted in DR of 28.0% (95% CI 14.3% to 47.6%) with sensitivity of 43.8% (95% CI 19.8% to 70.1%). Simon-Broome criteria had lower DR 11.3% (95% CI 6.0% to 20.0%) and specificity 70.9% (95% CI 64.8% to 76.5%) but higher sensitivity of 56.3% (95% CI 29.9% to 80.2%).
In primary care, in patients with cholesterol documented, FAMCAT 2 performs better than other case-finding criteria for detecting genetically confirmed FH, with no prior clinical review required for case finding.
NCT03934320.
家族性高胆固醇血症(FH)是一种常见的遗传性疾病,可导致早发性冠心病(CHD)和死亡。我们开发了一种新的家族性高胆固醇血症病例发现工具(FAMCAT 1)算法,用于初级保健,以提高 FH 的检出率。通过纳入早发性 CHD 的个人病史(FAMCAT 2 算法),进一步提高了该算法的性能。本研究评估了其在 95%特异性下检测一般人群中经基因证实的 FH 的性能。我们还比较了这些算法与既定的临床病例发现标准。
前瞻性验证研究,在 14 个普通诊所中,从胆固醇记录的普通成年人群中招募参与者。对于 260 名有可用健康记录的参与者,我们根据 FAMCAT 阈值、荷兰脂质诊所网络(DLCN)评分、Simon-Broome 标准和推荐的胆固醇阈值(总胆固醇> 9.0mmol/L,如果≥30 岁或> 7.5mmol/L,如果<30 岁),使用电子和手动提取患者记录和家族史问卷中的临床数据,确定可能的 FH 病例。参考标准是基因检测。我们检查了每种病例发现标准的检出率(DR)、敏感性和特异性。
在 95%特异性下,FAMCAT 1 的检出率为 27.8%(95%CI 12.5%至 50.9%),敏感性为 31.2%(95%CI 11.0%至 58.7%);而 FAMCAT 2 的检出率为 45.8%(95%CI 27.9%至 64.9%),敏感性为 68.8%(95%CI 41.3%至 89.0%)。DLCN 评分≥6 分的检出率为 35.3%(95%CI 17.3%至 58.7%),敏感性为 37.5%(95%CI 15.2%至 64.6%)。使用推荐的胆固醇阈值导致检出率为 28.0%(95%CI 14.3%至 47.6%),敏感性为 43.8%(95%CI 19.8%至 70.1%)。Simon-Broome 标准的检出率较低,为 11.3%(95%CI 6.0%至 20.0%),特异性较高,为 70.9%(95%CI 64.8%至 76.5%),但敏感性较高,为 56.3%(95%CI 29.9%至 80.2%)。
在初级保健中,对于有胆固醇记录的患者,FAMCAT 2 比其他病例发现标准在检测经基因证实的 FH 方面表现更好,无需事先进行临床评估。
NCT03934320。