Matthay Zachary A, Flanagan Colleen P, Sanders Katherine, Smith Eric J, Lancaster Elizabeth M, Gasper Warren J, Kornblith Lucy Z, Hiramoto Jade S, Conte Michael S, Iannuzzi James C
Department of Surgery, University of California, San Francisco, Calif.
Division of Vascular and Endovascular Surgery, Department of Surgery, University of California, San Francisco, Calif.
J Vasc Surg Venous Lymphat Disord. 2022 May;10(3):585-593.e2. doi: 10.1016/j.jvsv.2021.10.001. Epub 2021 Oct 9.
Venous thromboembolism (VTE) is an important cause of postoperative morbidity and mortality. However, the reported incidence after major vascular surgery has ranged from as low as 1% to >10%. Furthermore, little is known about optimal chemoprophylaxis regimens or rates of postdischarge VTE in this population. In the present study, we aimed to better characterize the rates of in-hospital and postdischarge VTE after major vascular surgery, the role of chemoprophylaxis timing, and the association of VTE with mortality.
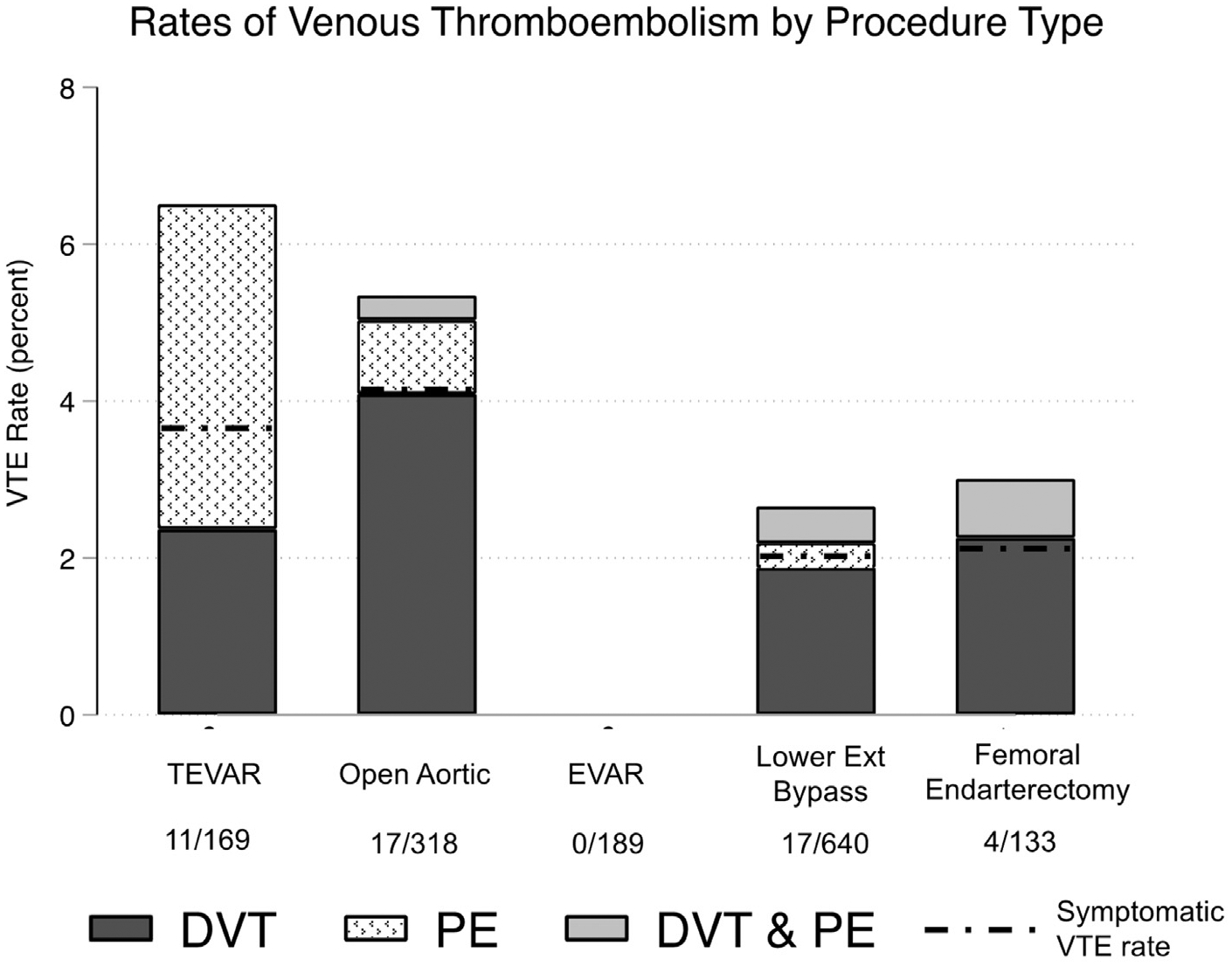
A single-center retrospective study of 1449 major vascular operations (2013-2020) was performed and included 189 endovascular abdominal aortic aneurysm repairs (13%), 169 thoracic endovascular aortic aneurysm repairs (12%), 318 open aortic operations (22%), 640 lower extremity bypasses (44%), and 133 femoral endarterectomies (9%). The baseline characteristics, anticoagulant and antiplatelet medications, and outcomes were abstracted from an electronic database with medical record auditing. Postoperative VTE (pulmonary embolism and deep vein thrombosis) within 90 days of surgery was classified by the location, symptoms, and treatment. A cut point analysis using Youden's index identified the most VTE discriminating timing of chemoprophylaxis (including therapeutic vs prophylactic anticoagulant and antiplatelet medications) and Caprini score. Multivariable logistic regression was used to test the association of VTE with chemoprophylaxis timing, Caprini score, and additional risk factors. Cox proportional hazard modeling was used to measure the association between VTE and mortality.
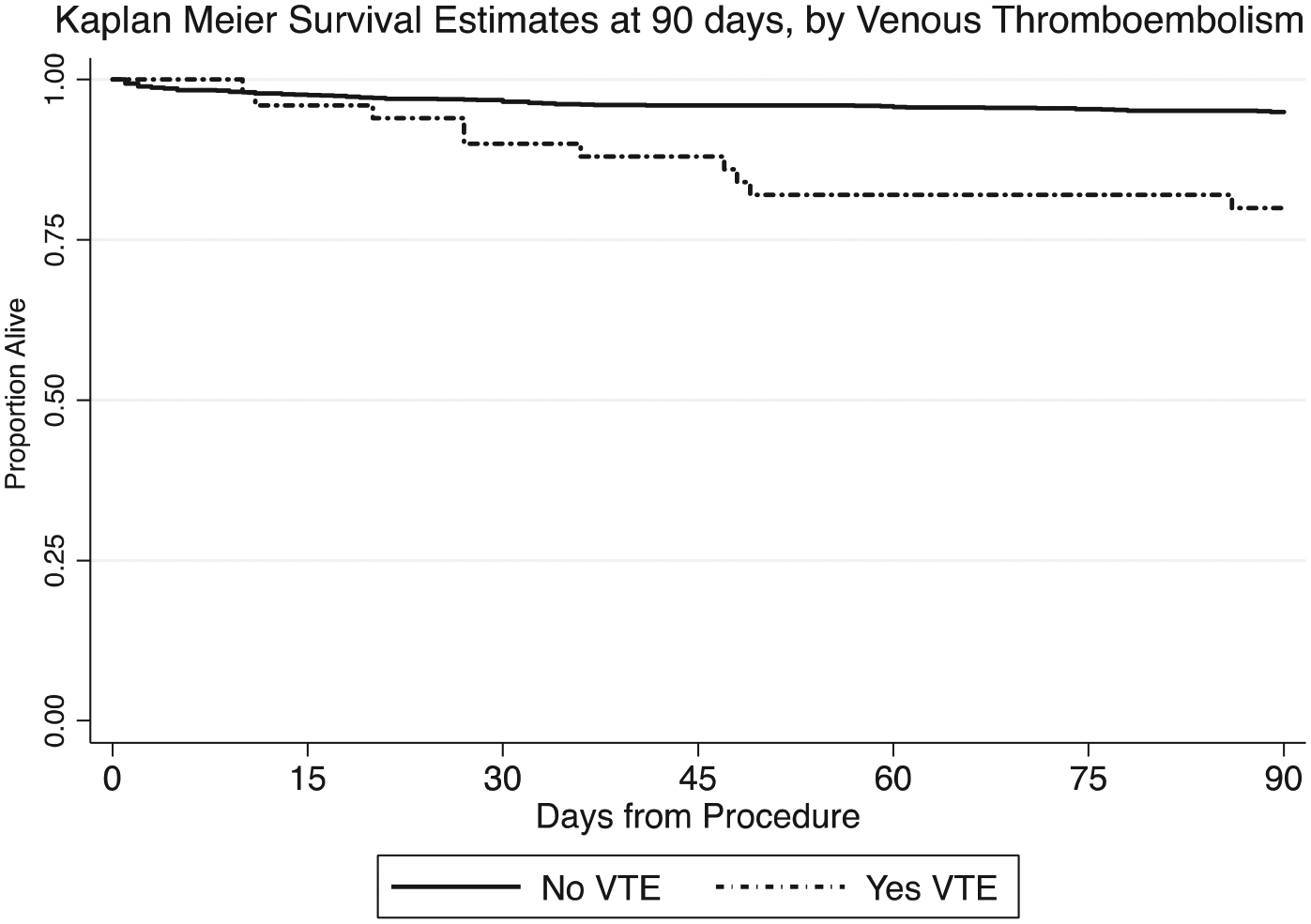
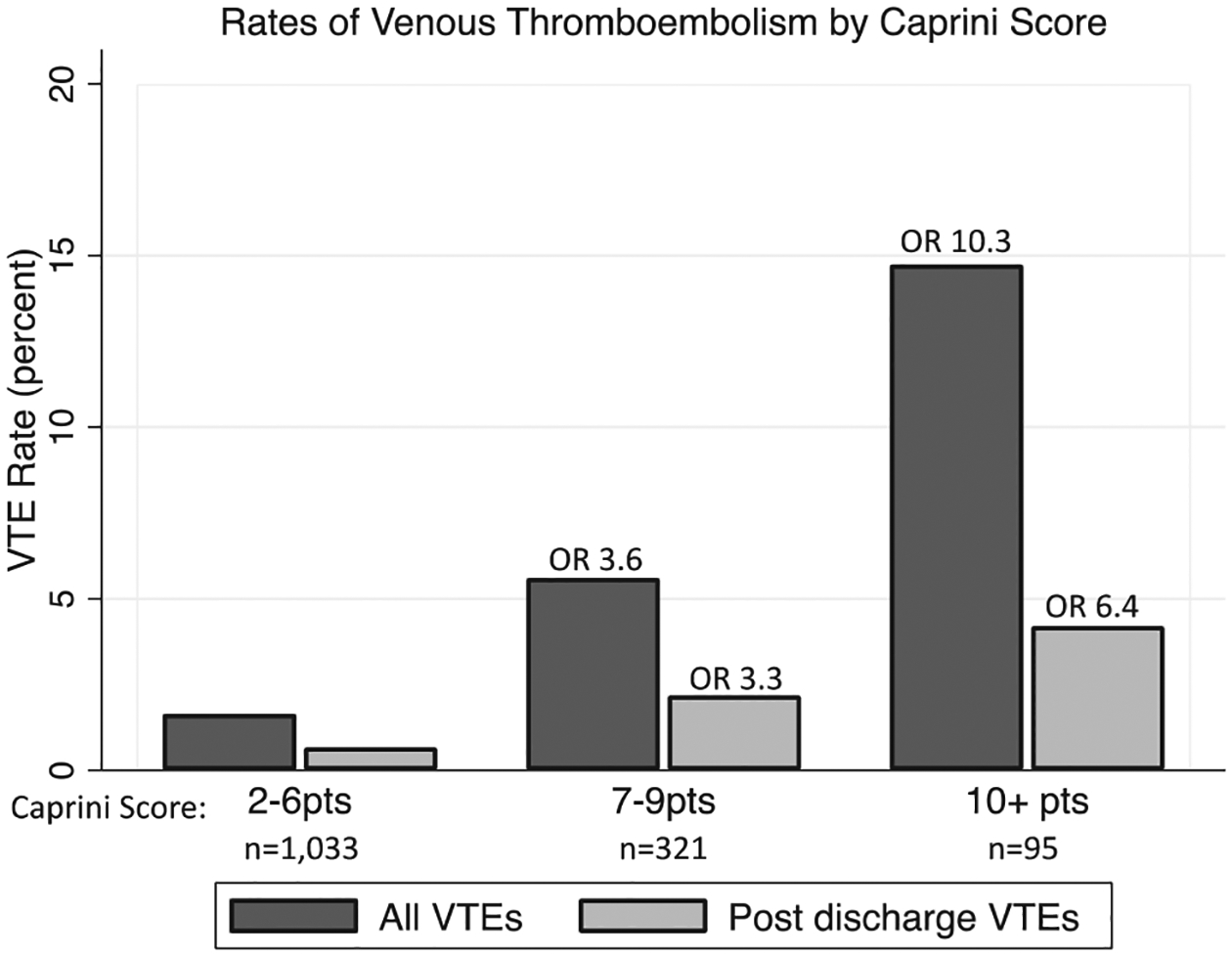
The overall VTE incidence was 3.4% (65% deep vein thrombosis; 25% pulmonary embolism; 10% both), and 37% had occurred after discharge. The rate of symptomatic VTE was 2.4%, which was lowest for endovascular abdominal aortic aneurysm repair (0.0%) and highest for open aortic surgery (4.1%; P = .02). Those who had developed VTE had had a longer length of stay, higher rates of end-stage renal disease and prior VTE, and higher Caprini scores (8 vs 5 points; P < .01 for all). Those who had developed VTE were also more likely to have received ≥2 U of blood postoperatively, required an unplanned return to the operating room, had delayed chemoprophylaxis, anticoagulation, and/or antiplatelet initiation of >4 days postoperatively, and had increased 90-day mortality (P < .01 for all). A Caprini score of ≥7 (29% of patients) was associated with postdischarge VTE (2.6% vs 0.7%; P = .01), and chemoprophylaxis, anticoagulation, and antiplatelet timing of >4 days was associated with an increased adjusted odds of VTE (odds ratio, 2.4; 95% confidence interval, 1.1-4.9). Although no fatal VTEs were identified, VTE was an independent predictor of 90-day mortality (adjusted hazard ratio, 2.7; 95% confidence interval, 1.3-5.9).
These data have shown that patients undergoing major vascular surgery are particularly prone to the development of VTE, with frequent hypercoagulable comorbidities. The earlier initiation of chemoprophylaxis was associated with a reduced risk of VTE development. Furthermore, the postdischarge VTE rates might reach thresholds warranting postdischarge chemoprophylaxis, especially for patients with a Caprini score of ≥7.
静脉血栓栓塞症(VTE)是术后发病和死亡的重要原因。然而,大血管手术后报告的发病率范围从低至1%到超过10%不等。此外,对于该人群中最佳的化学预防方案或出院后VTE发生率知之甚少。在本研究中,我们旨在更好地描述大血管手术后住院期间和出院后VTE的发生率、化学预防时机的作用以及VTE与死亡率的关联。
对1449例大血管手术(2013 - 2020年)进行单中心回顾性研究,包括189例腹主动脉瘤腔内修复术(13%)、169例胸主动脉瘤腔内修复术(12%)、318例开放性主动脉手术(22%)、640例下肢搭桥术(44%)和133例股动脉内膜切除术(9%)。从带有病历审核的电子数据库中提取基线特征、抗凝和抗血小板药物使用情况及结局。手术90天内的术后VTE(肺栓塞和深静脉血栓形成)根据部位、症状和治疗进行分类。使用尤登指数进行切点分析,确定化学预防(包括治疗性与预防性抗凝及抗血小板药物)和Caprini评分对VTE最具鉴别力的时机。采用多变量逻辑回归分析VTE与化学预防时机、Caprini评分及其他危险因素的关联。使用Cox比例风险模型测量VTE与死亡率之间的关联。
总体VTE发生率为3.4%(65%为深静脉血栓形成;25%为肺栓塞;10%两者皆有),37%发生在出院后。有症状VTE的发生率为2.4%,在腹主动脉瘤腔内修复术中最低(0.0%),在开放性主动脉手术中最高(4.1%;P = 0.02)。发生VTE的患者住院时间更长、终末期肾病和既往VTE发生率更高,Caprini评分更高(8分对5分;所有P < 0.01)。发生VTE的患者术后也更可能接受≥2单位输血、需要非计划性返回手术室、化学预防、抗凝和/或抗血小板治疗开始延迟超过术后4天,且90天死亡率增加(所有P < 0.01)。Caprini评分≥7(占患者的29%)与出院后VTE相关(2.6%对0.7%;P = 0.01),化学预防、抗凝和抗血小板治疗时机超过4天与VTE调整后发生几率增加相关(比值比,2.4;95%置信区间,1.1 - 4.9)。虽然未发现致命性VTE,但VTE是90天死亡率的独立预测因素(调整后风险比,2.7;95%置信区间,1.3 - 5.9)。
这些数据表明,接受大血管手术的患者特别容易发生VTE,且常伴有高凝合并症。更早开始化学预防与VTE发生风险降低相关。此外,出院后VTE发生率可能达到需要出院后化学预防的阈值,特别是对于Caprini评分≥7的患者。